You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Humerus FractureDocument20 pagesHumerus Fracturecaesaputri100% (1)
- Emergency Medicines List 2014Document38 pagesEmergency Medicines List 2014Michael Silva100% (3)
- Canadian Medical Residency GuideDocument239 pagesCanadian Medical Residency GuideSym Y100% (1)
- Joan Forsyth - Clinical Application of Mechanical Ventilation-White Press Academic (2018)Document253 pagesJoan Forsyth - Clinical Application of Mechanical Ventilation-White Press Academic (2018)Vlady78100% (1)
- Managing Health For Field Operations in Oil and Gas ActivitiesDocument44 pagesManaging Health For Field Operations in Oil and Gas Activitiesadeoye_okunoyeNo ratings yet
- Mod 3 Guidelines in Giving Emergency CAreDocument5 pagesMod 3 Guidelines in Giving Emergency CArerez1987100% (2)
- Idoc - Pub Rosen Medicina de Urgencias Tomo 1abbyyDocument994 pagesIdoc - Pub Rosen Medicina de Urgencias Tomo 1abbyyViviana González100% (1)
- Wound CareDocument14 pagesWound CareKirsten Padilla Chua100% (4)
- Bronze MedallionDocument2 pagesBronze Medallionearthmoon1No ratings yet
- Bone FracturesDocument21 pagesBone FracturesChintya Fidelia MontangNo ratings yet
- First Aid and Water SurvivalDocument4 pagesFirst Aid and Water SurvivalRobert MequilaNo ratings yet
- 2012 06 14 CENA - Position Statement TriageDocument5 pages2012 06 14 CENA - Position Statement TriageBudi KusumaNo ratings yet
- Base TestDocument28 pagesBase Testomarelbihi8No ratings yet
- Tubes NclexDocument3 pagesTubes NclexYoke W Khoo100% (1)
- First Aid InfoDocument9 pagesFirst Aid InfoHarrold CuteNo ratings yet
- What Is The Importance of CPRDocument3 pagesWhat Is The Importance of CPRapi-347101204100% (1)
- Color Code Look For Complied With ECE Look For With Partial Compliance, ECE Substitute Presented Look For Not CompliedDocument2 pagesColor Code Look For Complied With ECE Look For With Partial Compliance, ECE Substitute Presented Look For Not CompliedMelanie Nina ClareteNo ratings yet
- Morning Report Burn InjuryDocument27 pagesMorning Report Burn InjuryFebrian PutraNo ratings yet
- DFSGDFGDFDocument60 pagesDFSGDFGDFMada Dwi HariNo ratings yet
- Equipment List: Equipment and Supplies Quantity Needed Learning/Testing Station Equipment NeededDocument3 pagesEquipment List: Equipment and Supplies Quantity Needed Learning/Testing Station Equipment NeededVictoriano MendezNo ratings yet
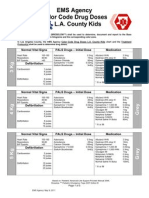
- EMS Agency Color Code Drug Doses L. L.A. County Kids: Normal Vital Signs PALS Drugs - Initial Dose MedicationDocument5 pagesEMS Agency Color Code Drug Doses L. L.A. County Kids: Normal Vital Signs PALS Drugs - Initial Dose MedicationCruz VerdeNo ratings yet
- Why Is CPR Important?Document7 pagesWhy Is CPR Important?Cake ManNo ratings yet
- Doctors Nurses Overcome Workplace HierarchiesDocument6 pagesDoctors Nurses Overcome Workplace HierarchiesAndres CarreraNo ratings yet
- AKU-NAMA - Summer 2009Document24 pagesAKU-NAMA - Summer 2009Abdul Basit SaeedNo ratings yet
- Basic Life Support (BLS)Document49 pagesBasic Life Support (BLS)Sukhbir KaurNo ratings yet
- Conversion of Crico To TrachDocument5 pagesConversion of Crico To Trachv_80185753No ratings yet
- NCMA219 Pedia CPR ChecklistDocument1 pageNCMA219 Pedia CPR ChecklistLumina lNo ratings yet
- Abdominal TraumaDocument20 pagesAbdominal TraumaSanthanu SukumaranNo ratings yet
- How To Treat A Bullet Wound (With Pictures) - WikiHowDocument7 pagesHow To Treat A Bullet Wound (With Pictures) - WikiHowOm Singh IndaNo ratings yet
- EFA DubaiDocument70 pagesEFA DubaiLifelinesafety ConsultantsNo ratings yet