You might also like
- Self Directive LearningDocument18 pagesSelf Directive Learningcrystal fate valdezNo ratings yet
- 1 MDW 204 Imci Integrated Management of Childhood IllnessDocument11 pages1 MDW 204 Imci Integrated Management of Childhood IllnessMaria Lejani TerencioNo ratings yet
- 7091371954mod 1 INTRODUCTION RDocument16 pages7091371954mod 1 INTRODUCTION RJEEJANo ratings yet
- Integrated Management of Neonatal and Childhood Illness Strategy An Approach For Hypothermia in NewbornsDocument5 pagesIntegrated Management of Neonatal and Childhood Illness Strategy An Approach For Hypothermia in NewbornsEditor IJTSRDNo ratings yet
- IMNCI Training Module 1-9Document356 pagesIMNCI Training Module 1-9smbawasaini50% (4)
- Childhood Obesity: Causes and Consequences, Prevention and Management.From EverandChildhood Obesity: Causes and Consequences, Prevention and Management.No ratings yet
- Pediatric Revieer PrelimsDocument3 pagesPediatric Revieer PrelimsJada GonzalesNo ratings yet
- Doh ProgramsDocument8 pagesDoh ProgramsClara CentineoNo ratings yet
- 1-Imci 48Document48 pages1-Imci 48Abdikadir MohamedNo ratings yet
- IMCIDocument11 pagesIMCIJoshua Villarba100% (1)
- SEMINAR ON ImnciDocument8 pagesSEMINAR ON Imncivineeta.ashoknagarNo ratings yet
- INTEGRATED MANAGEMENT OF NEONATE AND CHILDHOOD ILLNESS (Repaired)Document13 pagesINTEGRATED MANAGEMENT OF NEONATE AND CHILDHOOD ILLNESS (Repaired)Archana Sahu100% (2)
- Integrated Management of Childhood IllnessDocument3 pagesIntegrated Management of Childhood IllnessJanine Alexis BuenviajeNo ratings yet
- In The Pre-Hospital SettingDocument13 pagesIn The Pre-Hospital SettingMichael VillavertNo ratings yet
- Integrated Management of Childhood Illness (IMCI)Document10 pagesIntegrated Management of Childhood Illness (IMCI)Stephen Bona MinianoNo ratings yet
- EPI - AND - IMCI - Docx Filename - UTF-8''EPI AND IMCIDocument14 pagesEPI - AND - IMCI - Docx Filename - UTF-8''EPI AND IMCIYvonne Carmel Aguilar SunigaNo ratings yet
- DOH Programs Related To Family HealthDocument12 pagesDOH Programs Related To Family HealthSophia Nicole AranasNo ratings yet
- Weekly Activity Midterm CHN (Vivas, Mariah Jamby A. BSN-II)Document5 pagesWeekly Activity Midterm CHN (Vivas, Mariah Jamby A. BSN-II)Mariah VivasNo ratings yet
- Business DevelopemntDocument17 pagesBusiness Developemntayan ghoshNo ratings yet
- Report of Inservice EducationDocument35 pagesReport of Inservice EducationAkansha JohnNo ratings yet
- Integrated Management of Childhood IllnessDocument5 pagesIntegrated Management of Childhood IllnessheartianeNo ratings yet
- About Integrated Management of Childhood IllnessDocument5 pagesAbout Integrated Management of Childhood IllnessRouena Santiago VillaramaNo ratings yet
- Integrated Management On Childhood IllnessDocument3 pagesIntegrated Management On Childhood IllnessAbeer AguamNo ratings yet
- Jurnal AsiDocument15 pagesJurnal AsiAnastasiaNo ratings yet
- Imci - ChnfhaksDocument9 pagesImci - ChnfhaksvanessaNo ratings yet
- Integrated Management of Childhood IllnessDocument5 pagesIntegrated Management of Childhood Illnessjulieyauder624No ratings yet
- Factors Associated Early Termination of Exclusive Breastfeeding Among Infants Under Six MonthsDocument9 pagesFactors Associated Early Termination of Exclusive Breastfeeding Among Infants Under Six MonthsAmedo Hajji MohamedNo ratings yet
- Planning Implementing EvaluatingDocument213 pagesPlanning Implementing EvaluatingMichael John TahadlangitNo ratings yet
- Assesment of Infant and Young Child Feeding (IYCF) Practice - Policy and Programs in EthiopiaDocument42 pagesAssesment of Infant and Young Child Feeding (IYCF) Practice - Policy and Programs in Ethiopiatsehaiassefa100% (1)
- Integrated Management of Childhood IllnessDocument18 pagesIntegrated Management of Childhood IllnessRika Mae100% (1)
- By: 1. Alaa Yousif Dafalla 2. Reham Hamad Mohamed 3. Abubaker Mahmoud MohamedDocument31 pagesBy: 1. Alaa Yousif Dafalla 2. Reham Hamad Mohamed 3. Abubaker Mahmoud MohamedAhmed AlbagerNo ratings yet
- 1 IMCI IntroductionDocument13 pages1 IMCI IntroductionESTE CRECIA EDULLANTES BULLECERNo ratings yet
- E Inc PoliciesDocument2 pagesE Inc PoliciesricogeminaNo ratings yet
- Growth Chart and Care of Under Five ChildrenDocument31 pagesGrowth Chart and Care of Under Five ChildrenWek KivNo ratings yet
- The Integrated Management of Childhood IllnessesDocument32 pagesThe Integrated Management of Childhood IllnessesKrishna PhulpagarNo ratings yet
- Integrated Management of Childhood Illness (IMCI)Document48 pagesIntegrated Management of Childhood Illness (IMCI)Ram krishnaNo ratings yet
- Moyo Wa Bana: A Novel Approach To Reducing Child Mortality in ZambiaDocument40 pagesMoyo Wa Bana: A Novel Approach To Reducing Child Mortality in ZambiaCAREZAMBIANo ratings yet
- Untitled DocumentDocument3 pagesUntitled DocumentKhenyuza Angel ClementeNo ratings yet
- Doh Health Programs 1Document139 pagesDoh Health Programs 1Eric VeranoNo ratings yet
- Session 1 MBFHI A Part of Global Strateegy of MBFHIDocument32 pagesSession 1 MBFHI A Part of Global Strateegy of MBFHItitatabujaraNo ratings yet
- S1 IntroductionDocument17 pagesS1 IntroductionBelay GezahegnNo ratings yet
- Joaquim Pinto, Lic - SP, M.M, M.MTSC, DR. Lidia Gomes SKM, MPH, Dr. Avelino Guterres Correia, MPH, Ministry of Health of Timor-LesteDocument7 pagesJoaquim Pinto, Lic - SP, M.M, M.MTSC, DR. Lidia Gomes SKM, MPH, Dr. Avelino Guterres Correia, MPH, Ministry of Health of Timor-LesteInternational Journal of Innovative Science and Research Technology100% (1)
- AO 2009 0025 Essential Newborn CareDocument15 pagesAO 2009 0025 Essential Newborn Carejulesubayubay542895% (21)
- Commed Imci PedroDocument5 pagesCommed Imci PedroMaria Nerissa ToledoNo ratings yet
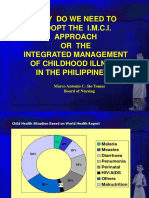
- Why Do We Need To Adopt The I.M.C.I. Approach or The Integrated Management of Childhood Illness in The Philippines ?Document15 pagesWhy Do We Need To Adopt The I.M.C.I. Approach or The Integrated Management of Childhood Illness in The Philippines ?Mae DoctoleroNo ratings yet
- Febrile Illness 2019 Shamim QaziDocument27 pagesFebrile Illness 2019 Shamim QaziAbdi TofikNo ratings yet
- BreastfeedDocument5 pagesBreastfeedBetHsy Pascua100% (1)
- IMCIDocument15 pagesIMCISandy JusiNo ratings yet
- Hes 409, Week 1-3Document9 pagesHes 409, Week 1-3sodiqajayi2018No ratings yet
- Integrated Management of Childhood IllnessDocument13 pagesIntegrated Management of Childhood IllnessRachelle Gay PacialNo ratings yet
- Rate of Exclusive Breastfeeding Among Postpartum Mothers at Hoima Regional Referral Hospital's Postnatal ClinicDocument13 pagesRate of Exclusive Breastfeeding Among Postpartum Mothers at Hoima Regional Referral Hospital's Postnatal ClinicKIU PUBLICATION AND EXTENSIONNo ratings yet
- Integrated Management of Childhood IllnessDocument8 pagesIntegrated Management of Childhood IllnessSehar162No ratings yet
- MCN Lecture NotesDocument52 pagesMCN Lecture NotesJHYANE KYLA TRILLESNo ratings yet
- Overview & Community Pediatrics: DefinitionDocument3 pagesOverview & Community Pediatrics: DefinitionJessica Febrina WuisanNo ratings yet
- Millions Saved: New Cases of Proven Success in Global HealthFrom EverandMillions Saved: New Cases of Proven Success in Global HealthRating: 5 out of 5 stars5/5 (1)
- Well-Child Care in Infancy: Promoting Readiness for LifeFrom EverandWell-Child Care in Infancy: Promoting Readiness for LifeNo ratings yet
- Building Future Health and Well-Being of Thriving Toddlers and Young Children: 95th Nestlé Nutrition Institute Workshop, September 2020From EverandBuilding Future Health and Well-Being of Thriving Toddlers and Young Children: 95th Nestlé Nutrition Institute Workshop, September 2020No ratings yet
- Hes 008 - Sas 22Document1 pageHes 008 - Sas 22Juliannah ColinaresNo ratings yet
- Medical ManualDocument144 pagesMedical ManualDevinder Singh50% (2)
- Research Proposal For NurseDocument44 pagesResearch Proposal For Nursefiraolab5No ratings yet
- Jarvis Physical Examination Health Assessment Chap - 01Document18 pagesJarvis Physical Examination Health Assessment Chap - 01Don Rivetts94% (18)
- The Catholic University of Korea, Seoul St. Mary's Hospital: Contact PointDocument1 pageThe Catholic University of Korea, Seoul St. Mary's Hospital: Contact PointAhmed AlhadiNo ratings yet
- Infant Bacterial TherapeuticsDocument67 pagesInfant Bacterial TherapeuticsSuki HanantoNo ratings yet
- Kord Butler Letter To GovDocument3 pagesKord Butler Letter To Govapi-617724507No ratings yet
- Standards For Nursing EducationDocument7 pagesStandards For Nursing Educationemir_bautista2002No ratings yet
- OsteosarcomaDocument5 pagesOsteosarcomaEnrico LeonartoNo ratings yet
- Health Care Payment PDFDocument174 pagesHealth Care Payment PDFAshri Nur IstiqomahNo ratings yet
- What Is Next After Passing The Board ExamDocument6 pagesWhat Is Next After Passing The Board Examtimie_reyesNo ratings yet
- Oxford Handbook of General PracticeDocument5 pagesOxford Handbook of General PracticeMohammed AhmmedNo ratings yet
- IC 38 GI Question BankDocument40 pagesIC 38 GI Question BankShilpy KaurNo ratings yet
- Unit I - Introduction-to-Midwifery-Obstetrical-NursingDocument43 pagesUnit I - Introduction-to-Midwifery-Obstetrical-NursingN. Siva100% (8)
- IDCRP Brown Bag Presentation - CRF - 26feb2015Document33 pagesIDCRP Brown Bag Presentation - CRF - 26feb2015shivam singhNo ratings yet
- hw499 Unit 2 SyllabusDocument2 pageshw499 Unit 2 Syllabusapi-662078826No ratings yet
- (Family Nursing Care Plan) - 2Document3 pages(Family Nursing Care Plan) - 2Pilar 'Phie' S. Caparas100% (1)
- Quality and Safety Walk Rounds A Co Designed Approach Toolkit and Case Study ReportDocument52 pagesQuality and Safety Walk Rounds A Co Designed Approach Toolkit and Case Study ReportFederico GorgasNo ratings yet
- Application of Bioethical PrinciplesDocument1 pageApplication of Bioethical PrinciplesnichollelucrenzeNo ratings yet
- Modern College of Pharmacy, Khurd (Sangrur) : Practical Training Contract Form For PharmacistDocument1 pageModern College of Pharmacy, Khurd (Sangrur) : Practical Training Contract Form For PharmacistModern College KhurdNo ratings yet
- Course Information For Current Semester/Term: Maklumat Kursus Untuk Semester/Penggal SemasaDocument5 pagesCourse Information For Current Semester/Term: Maklumat Kursus Untuk Semester/Penggal SemasaNurul IrhamnaNo ratings yet
- Optical BranchDocument6 pagesOptical Branchmmdumullana03No ratings yet
- AnnexG eKAS&ePresSDocument2 pagesAnnexG eKAS&ePresSLaish Christle CapiendoNo ratings yet
- Emergency Patient Assessment FormDocument2 pagesEmergency Patient Assessment Formmohamed elgabryNo ratings yet
- Sexual Transmitted Diseases LessonDocument33 pagesSexual Transmitted Diseases LessonYonaNo ratings yet
- Hip Fractures-Orthoinfo - AaosDocument9 pagesHip Fractures-Orthoinfo - Aaosapi-228773845No ratings yet
- Case ScenarioDocument3 pagesCase ScenarioKhyress Kyla BalalaNo ratings yet
- CQC Standards Easy Format v2Document29 pagesCQC Standards Easy Format v2Simply Health and SafetyNo ratings yet
- Annex2 Website1702151655Document126 pagesAnnex2 Website1702151655Muhammad Fakhar AbbasNo ratings yet
- MASTER IN HEALTH ADMIINISTRATION IN UNCC, AmericaDocument52 pagesMASTER IN HEALTH ADMIINISTRATION IN UNCC, AmericaRandom RajNo ratings yet