You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Breast Unit SOP: Checklist While Giving ROIS AppointmentDocument7 pagesBreast Unit SOP: Checklist While Giving ROIS AppointmentAbhinav Ingle100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Health Referral System Manual - Central VisayasDocument103 pagesHealth Referral System Manual - Central VisayasAlfred Russel Wallace50% (10)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- A Simple Technique To Measure The Volume of Removed Buccal FatDocument3 pagesA Simple Technique To Measure The Volume of Removed Buccal FatGuilherme GuerraNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Updates in Ophthalmic Anaesthesia in AdultsDocument7 pagesUpdates in Ophthalmic Anaesthesia in AdultsJossiel OlivaresNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Clinical Application of Nightingale TheoryDocument9 pagesClinical Application of Nightingale TheoryHina Nizar100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- To Evaluate The Efficacy of Ultrasonography Guided Pectoral Nerve Block For Postoperative Analgesia in Breast SurgeriesDocument4 pagesTo Evaluate The Efficacy of Ultrasonography Guided Pectoral Nerve Block For Postoperative Analgesia in Breast SurgeriesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Batu Ren, Batu Ureter Dan Onko NewDocument29 pagesBatu Ren, Batu Ureter Dan Onko Newilham masdarNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Revised Dentist (Code Od Ethics) Regulations, 2014 PDFDocument10 pagesThe Revised Dentist (Code Od Ethics) Regulations, 2014 PDFRohit AgrawalNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- 279667.locs IiiDocument16 pages279667.locs IiiSiomay IkanNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Tam MannaDocument2 pagesTam MannaYashwanth GowdaNo ratings yet
- Como Analizar Un ArticuloDocument4 pagesComo Analizar Un ArticuloAlvaro Alvarez RiveraNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Career GuidanceDocument19 pagesCareer GuidanceAbdul JalilNo ratings yet
- General Surgery&plastic Surgery Board-Part One Exam Blueprint (v.1)Document4 pagesGeneral Surgery&plastic Surgery Board-Part One Exam Blueprint (v.1)Mohammed S. Al Ghamdi100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 4.2 MDS01 - Definition Table of The MDS Items - Ver0.94Document7 pages4.2 MDS01 - Definition Table of The MDS Items - Ver0.94AriniDwiLestariNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Operating Room ConceptsDocument47 pagesOperating Room ConceptsLoungayvan Batuyog100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
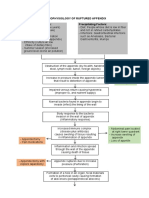
- Pathophysiology of Ruptured AppendixDocument2 pagesPathophysiology of Ruptured AppendixAya PaquitNo ratings yet
- Minor Surgical Procedures in Maxillofacial SurgeryDocument65 pagesMinor Surgical Procedures in Maxillofacial SurgerydrzibranNo ratings yet
- Hubungan Tindakan Perawatan Luka Dengan f8dc88cdDocument8 pagesHubungan Tindakan Perawatan Luka Dengan f8dc88cdRD OfficialNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Incisions January June 2014Document40 pagesIncisions January June 2014Raine Bow100% (1)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Financial Planning and ForecastingDocument6 pagesFinancial Planning and ForecastingMaryam UmairNo ratings yet
- ERAS - ProtocolDocument5 pagesERAS - ProtocolShakya WeeraratneNo ratings yet
- Daftar Harga Indosopha 2012 Bp. Edward Roy Palangkaraya PDFDocument5 pagesDaftar Harga Indosopha 2012 Bp. Edward Roy Palangkaraya PDFBoyke WinterbergNo ratings yet
- NCLEX Test Questions With RationaleDocument46 pagesNCLEX Test Questions With Rationaletetmetrangmail.com tet101486No ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Cleft Lip and Palate: Current Surgical ManagementDocument3 pagesCleft Lip and Palate: Current Surgical ManagementFarisa BelaNo ratings yet
- Organizational Structure - ApolloDocument13 pagesOrganizational Structure - ApolloIpreetponnamma86% (7)
- MediCAD Brochure 2D + 3D (Except Shoulder)Document16 pagesMediCAD Brochure 2D + 3D (Except Shoulder)kocis_pNo ratings yet
- Isjna Vol 17 2 Summer 2018Document72 pagesIsjna Vol 17 2 Summer 2018Nissa KurniaNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- CH 5Document153 pagesCH 5sojithesouljaNo ratings yet
- 5.2spatial Translations Administrative Office Matrix DiagramDocument3 pages5.2spatial Translations Administrative Office Matrix DiagramAthena AciboNo ratings yet
- Exam 2Document4 pagesExam 2Azra MuzafarNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)