You might also like
- Military Triag ADocument14 pagesMilitary Triag Asupit1No ratings yet
- Heart Views-Cardio GlicemicDocument24 pagesHeart Views-Cardio Glicemicsupit1No ratings yet
- Heart Views-Ghrelin CardioprotectiveDocument6 pagesHeart Views-Ghrelin Cardioprotectivesupit1No ratings yet
- Journal TB RadiologyDocument13 pagesJournal TB Radiologysupit1No ratings yet
- Cerebellopontine Angle AnatomiDocument2 pagesCerebellopontine Angle Anatomisupit1No ratings yet
- Jurnal Shivering Post OpDocument7 pagesJurnal Shivering Post Opsupit1No ratings yet
- Guideline HF 2013Document79 pagesGuideline HF 2013supit1No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Neuro Tract Lesions Ps230114Document16 pagesNeuro Tract Lesions Ps230114সোমনাথ মহাপাত্রNo ratings yet
- Bone Anchored Maxillary Protraction 2012 American Journal of Orthodontics and Dentofacial OrthopedicsDocument2 pagesBone Anchored Maxillary Protraction 2012 American Journal of Orthodontics and Dentofacial OrthopedicsjosemtzzNo ratings yet
- PV Loop PresentationDocument25 pagesPV Loop PresentationAshish PandeyNo ratings yet
- June Free Chapter - The Tools by Phil Stutz and Barry MichelsDocument26 pagesJune Free Chapter - The Tools by Phil Stutz and Barry MichelsRandomHouseAU88% (17)
- Anna's HerbalDocument71 pagesAnna's Herbalhari haraNo ratings yet
- Malingering in Ophthalmology TestDocument7 pagesMalingering in Ophthalmology TestmasmedicaNo ratings yet
- Print Expected Seat Matrix TamilnaduDocument2 pagesPrint Expected Seat Matrix TamilnaduAshok PaskalrajNo ratings yet
- Medical Therapy Versus Balloon Sinus Dilation in Adults With Chronic Rhinosinusitis (MERLOT) : 12-Month Follow-UpDocument9 pagesMedical Therapy Versus Balloon Sinus Dilation in Adults With Chronic Rhinosinusitis (MERLOT) : 12-Month Follow-UpNevyNo ratings yet
- Edema: USMLE Step 1 Web Prep - Circulatory PathologyDocument9 pagesEdema: USMLE Step 1 Web Prep - Circulatory PathologyfrabziNo ratings yet
- Azygos Venos System 2Document17 pagesAzygos Venos System 2Fazil Omar BelwaelNo ratings yet
- Ankle-Brachial Index For Assessment of Peripheral Arterial DiseaseDocument5 pagesAnkle-Brachial Index For Assessment of Peripheral Arterial DiseaseindrawepeNo ratings yet
- Chronic Hepatitis BDocument9 pagesChronic Hepatitis Bmits98No ratings yet
- Offshore Survival Course and MedicalsDocument3 pagesOffshore Survival Course and MedicalsRony LesbtNo ratings yet
- Neinsteins Adolescent and Young Adult Health Care A Practical Guide Ebook PDF VersionDocument62 pagesNeinsteins Adolescent and Young Adult Health Care A Practical Guide Ebook PDF Versioneleanor.gamble412100% (45)
- Legg Calvé Perthes DiseaseDocument11 pagesLegg Calvé Perthes DiseaseronnyNo ratings yet
- Modern Endodontic PracticeDocument335 pagesModern Endodontic PracticeMiguel Jaèn100% (1)
- Integrating ReflexesDocument2 pagesIntegrating ReflexesAbigail Tan100% (2)
- Effect of Kangaroo Mother Care On Weight Gain in Low Birth Weight BabiesDocument21 pagesEffect of Kangaroo Mother Care On Weight Gain in Low Birth Weight BabiesTHONDYNALUNo ratings yet
- NA-0201 Application For Driving Licence and Certificate of Professional Competence (In English)Document2 pagesNA-0201 Application For Driving Licence and Certificate of Professional Competence (In English)Del MabelNo ratings yet
- Hero of ObgDocument2 pagesHero of ObgAnish VeettiyankalNo ratings yet
- Physiology System Specific Physiology (399Qs)Document170 pagesPhysiology System Specific Physiology (399Qs)rajvikram87No ratings yet
- Updated For 75 BDSDocument55 pagesUpdated For 75 BDSArfanNo ratings yet
- Nihon Kohden Tec-5531EDocument137 pagesNihon Kohden Tec-5531EDanniel Schaaf100% (1)
- GBS MeningitisDocument3 pagesGBS MeningitisMahmoud AbouelsoudNo ratings yet
- Complaint: Commissioner@afp - Gov.au Acv@health - Gov.au Committees@health - Gov.auDocument40 pagesComplaint: Commissioner@afp - Gov.au Acv@health - Gov.au Committees@health - Gov.auGerrit Hendrik Schorel-HlavkaNo ratings yet
- Handouts Echo Essentials Echo Cheat SheetDocument5 pagesHandouts Echo Essentials Echo Cheat Sheetadelina052008No ratings yet
- Easy Oral Motor Exercises To TryDocument4 pagesEasy Oral Motor Exercises To TryAzryanty Mohamad ArifinNo ratings yet
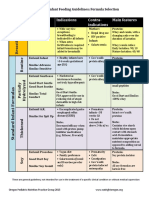
- Formula Selection OPNPGDocument2 pagesFormula Selection OPNPGRina PratiwiNo ratings yet
- Hemangioma Oral (Gill)Document4 pagesHemangioma Oral (Gill)koizorabigNo ratings yet
- Sebazole PISDocument2 pagesSebazole PISAstuti PrimadaniNo ratings yet