You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Criteria of SelectionDocument12 pagesCriteria of SelectionVinisha Vipin SharmaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Diff Betwn Inlay and Amalgam CavityDocument7 pagesDiff Betwn Inlay and Amalgam CavityVinisha Vipin Sharma100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Non Surgical Management of Periapical Lesions Using Calcium HydroxideDocument6 pagesNon Surgical Management of Periapical Lesions Using Calcium HydroxideVinisha Vipin SharmaNo ratings yet
- Some Basics of LasersDocument102 pagesSome Basics of LasersVinisha Vipin SharmaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Challenges in Working Length DeterminationDocument101 pagesChallenges in Working Length DeterminationVinisha Vipin SharmaNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Acupuncture in Dentistry PDFDocument73 pagesAcupuncture in Dentistry PDFVinisha Vipin SharmaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Mechanical Preparation Updated May2017 Prof Marco VersianiDocument159 pagesMechanical Preparation Updated May2017 Prof Marco VersianiVinisha Vipin SharmaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Laser in Conservative Dentistry & EndodonticsDocument75 pagesLaser in Conservative Dentistry & EndodonticsVinisha Vipin SharmaNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Eaat 14 I 1 P 217Document6 pagesEaat 14 I 1 P 217Vinisha Vipin SharmaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Content ServerDocument5 pagesContent ServerVinisha Vipin SharmaNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Content ServerDocument6 pagesContent ServerVinisha Vipin SharmaNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Glide Path PreparationDocument5 pagesGlide Path PreparationVinisha Vipin SharmaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Show TextDocument1 pageShow TextVinisha Vipin SharmaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- EchsDocument20 pagesEchsVinisha Vipin SharmaNo ratings yet
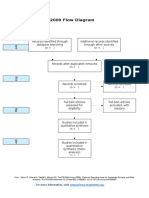
- PRISMA 2009 Flow Diagram: For More Information, VisitDocument1 pagePRISMA 2009 Flow Diagram: For More Information, VisitVinisha Vipin SharmaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Practice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportDocument5 pagesPractice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportVinisha Vipin SharmaNo ratings yet
- Ceramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveDocument5 pagesCeramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveVinisha Vipin SharmaNo ratings yet
- Dentin HypersensitivityDocument62 pagesDentin HypersensitivityVinisha Vipin Sharma100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Nanodentistry: New Buzz in Dentistry: Review ArticleDocument5 pagesNanodentistry: New Buzz in Dentistry: Review ArticleVinisha Vipin SharmaNo ratings yet
- PRISMA-P Statement - Moher Sys Rev Jan 2015Document9 pagesPRISMA-P Statement - Moher Sys Rev Jan 2015Vinisha Vipin SharmaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Clarks Cavity PreparationDocument10 pagesClarks Cavity PreparationVinisha Vipin SharmaNo ratings yet
- Pin Retained RestorationDocument31 pagesPin Retained RestorationVinisha Vipin SharmaNo ratings yet
- Esthetic Alternatives To AmalgamDocument15 pagesEsthetic Alternatives To AmalgamVinisha Vipin SharmaNo ratings yet
- Data Sheet: Experiment 1: Chemical ReactionsDocument17 pagesData Sheet: Experiment 1: Chemical ReactionsLinh NguyễnNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Brusseau, M. L., & Artiola, J. F. (2019) - Chemical Contaminants. in Environmental and Pollution Science (Pp. 175-190) - Academic Press.Document16 pagesBrusseau, M. L., & Artiola, J. F. (2019) - Chemical Contaminants. in Environmental and Pollution Science (Pp. 175-190) - Academic Press.Jimena ValeriaNo ratings yet
- Sae j429 Vs Astm A354 BD PDFDocument2 pagesSae j429 Vs Astm A354 BD PDFAdam GordonNo ratings yet
- SXK New Price ListDocument5 pagesSXK New Price ListidchandraNo ratings yet
- Plastic InjectionDocument39 pagesPlastic InjectionRishav KumarNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Komposit UHMWPE Sebagai Alternatif Bantalan Rel Kereta Api: Abel Evan, Alia Kristika, Farid Mulia LatiefDocument11 pagesKomposit UHMWPE Sebagai Alternatif Bantalan Rel Kereta Api: Abel Evan, Alia Kristika, Farid Mulia LatiefAlia KristikaNo ratings yet
- SN 200Document100 pagesSN 200T Mathew Tholoor100% (2)
- Water Cement RatioDocument5 pagesWater Cement RatioCastro FarfansNo ratings yet
- Paper 2 Paper With Solution ChemistryDocument14 pagesPaper 2 Paper With Solution ChemistryddssdsfsNo ratings yet
- Powder Coating Expert - VoicesDocument2 pagesPowder Coating Expert - VoicesChinmoy DholeNo ratings yet
- Timer PaperDocument5 pagesTimer Paperhajjiyare2016No ratings yet
- Experiments To WriteDocument53 pagesExperiments To WriteSUMAIRA ALTAFNo ratings yet
- For Bolstering Concrete: Panicum Maximum Jacq. Ash and Pulverized Corbicula Fluminea As An AdmixtureDocument4 pagesFor Bolstering Concrete: Panicum Maximum Jacq. Ash and Pulverized Corbicula Fluminea As An AdmixtureKristianKurtRicaroNo ratings yet
- Microstructure and Mechanical Properties of Low Carbon Steel WiresDocument8 pagesMicrostructure and Mechanical Properties of Low Carbon Steel WiresLeonardo ZarateNo ratings yet
- Termolisis PDFDocument16 pagesTermolisis PDFGaby Taipe AndaguaNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Chem Topic 8 PracticeDocument8 pagesChem Topic 8 Practicekakahem246No ratings yet
- Janchik R Lost Circulation Solutions For Lime Stones and Induced FracturesDocument23 pagesJanchik R Lost Circulation Solutions For Lime Stones and Induced FracturesVarun DodhiaNo ratings yet
- International CataloguesDocument18 pagesInternational CataloguesHuy ThaiNo ratings yet
- Ajilima 395 ReportDocument8 pagesAjilima 395 ReportLionel ZaysonNo ratings yet
- Pinnacle Flo, InC.Document16 pagesPinnacle Flo, InC.r_chulinNo ratings yet
- Determination of Length Change of Concrete Due To Alkali-Silica ReactionDocument7 pagesDetermination of Length Change of Concrete Due To Alkali-Silica Reactioniipmnpti iipm100% (1)
- NGL CT 1 0000 Pi SP 2013 D1 PDFDocument21 pagesNGL CT 1 0000 Pi SP 2013 D1 PDFAnonymous cVnKDdhNo ratings yet
- DJDocument8 pagesDJDiego JaquesNo ratings yet
- Joseph Abrusci - Professional Homemade Cherry BombsDocument26 pagesJoseph Abrusci - Professional Homemade Cherry BombsLê Nguyên ĐứcNo ratings yet
- Torsion: Torsional ReinforcingDocument9 pagesTorsion: Torsional ReinforcingRuel ElidoNo ratings yet
- Metamorphic Rocks PracticalDocument27 pagesMetamorphic Rocks PracticalMr Gk meenaNo ratings yet
- Topic 7Document39 pagesTopic 7deema dmdNo ratings yet
- (Lec6) Phase EquilibriaDocument52 pages(Lec6) Phase EquilibriadinurjNo ratings yet
- PSA Valves CriticalDesignFeatures MARKEDDocument41 pagesPSA Valves CriticalDesignFeatures MARKEDdj22500No ratings yet
- Mechanical Properties: Issues To Address..Document40 pagesMechanical Properties: Issues To Address..Mat MatttNo ratings yet
- Sodium Bicarbonate: Nature's Unique First Aid RemedyFrom EverandSodium Bicarbonate: Nature's Unique First Aid RemedyRating: 5 out of 5 stars5/5 (21)
- Periodic Tales: A Cultural History of the Elements, from Arsenic to ZincFrom EverandPeriodic Tales: A Cultural History of the Elements, from Arsenic to ZincRating: 3.5 out of 5 stars3.5/5 (137)
- Process Plant Equipment: Operation, Control, and ReliabilityFrom EverandProcess Plant Equipment: Operation, Control, and ReliabilityRating: 5 out of 5 stars5/5 (1)
- The Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactFrom EverandThe Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactRating: 5 out of 5 stars5/5 (5)