You might also like
- Disfagia NeurologicalsciencesDocument4 pagesDisfagia NeurologicalsciencesVaneciaBellaNo ratings yet
- Disfagia NeurologicalsciencesDocument4 pagesDisfagia NeurologicalsciencesVaneciaBellaNo ratings yet
- Gambaran Virus Hepatitis BDocument1 pageGambaran Virus Hepatitis BVaneciaBellaNo ratings yet
- 222 456 1 PBDocument7 pages222 456 1 PBmuh_nabil1838No ratings yet
- Phsyiology of Digestive SystemDocument2 pagesPhsyiology of Digestive SystemVaneciaBellaNo ratings yet
- Digestive System of HumanDocument3 pagesDigestive System of HumanVaneciaBellaNo ratings yet
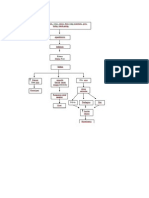
- Pathway AppendisitisDocument1 pagePathway AppendisitisVaneciaBellaNo ratings yet
- Enggorment PayudaraDocument66 pagesEnggorment PayudaraVaneciaBellaNo ratings yet
- Engorgment Pasca SalinDocument15 pagesEngorgment Pasca SalinVaneciaBellaNo ratings yet
- CH 8 Normal and Abnormal Post PartumDocument124 pagesCH 8 Normal and Abnormal Post PartumVaneciaBellaNo ratings yet
- Enggorment PayudaraDocument66 pagesEnggorment PayudaraVaneciaBellaNo ratings yet
- Hernia: RSST Klaten Koas Stase Bedah A13.1Document54 pagesHernia: RSST Klaten Koas Stase Bedah A13.1Bagus WirayudaNo ratings yet
- Hernia: RSST Klaten Koas Stase Bedah A13.1Document54 pagesHernia: RSST Klaten Koas Stase Bedah A13.1Bagus WirayudaNo ratings yet
- PP CompDocument66 pagesPP CompVaneciaBellaNo ratings yet
- Cervical Vulva R Cancer 2012Document63 pagesCervical Vulva R Cancer 2012VaneciaBellaNo ratings yet
- CervixCheck Brief PowerPoint Sep11Document16 pagesCervixCheck Brief PowerPoint Sep11VaneciaBellaNo ratings yet
- Buku Pedoman Nasional Penanggulangan TBCDocument131 pagesBuku Pedoman Nasional Penanggulangan TBCHasrapriliana Hersya100% (1)
- Breast Feeding and Its Associated ComplicationsDocument43 pagesBreast Feeding and Its Associated ComplicationsVaneciaBellaNo ratings yet
- PP CompDocument66 pagesPP CompVaneciaBellaNo ratings yet
- CH 8 Normal and Abnormal Post PartumDocument124 pagesCH 8 Normal and Abnormal Post PartumVaneciaBellaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- HAAD ReviewerDocument27 pagesHAAD Reviewerkimberly timbalNo ratings yet
- Tabel FMSPADocument6 pagesTabel FMSPAMumtaz MaulanaNo ratings yet
- HypertensionDocument23 pagesHypertensionrey magsayoNo ratings yet
- Hypertensive Emergency, El - ShahawyDocument41 pagesHypertensive Emergency, El - ShahawysalwaNo ratings yet
- PamphletDocument2 pagesPamphletapi-25931970033% (3)
- Ob 2Document17 pagesOb 2Rizza Mae SalvaniaNo ratings yet
- Case Based Discussion: Non-PsychoticDocument40 pagesCase Based Discussion: Non-PsychoticIvana Ester Sinta UliNo ratings yet
- Arterias FacialesDocument23 pagesArterias FacialesDaniela GonzalezNo ratings yet
- Neurological ConditionsDocument7 pagesNeurological ConditionsitayNo ratings yet
- HOPE: Health Optimizing Physical EducationDocument41 pagesHOPE: Health Optimizing Physical Educationjoe blowNo ratings yet
- Aapher Physical Fitness Test: S.No Test Items ProposeDocument15 pagesAapher Physical Fitness Test: S.No Test Items ProposeS. VeeravelNo ratings yet
- Drug Study: METOPROLOL: Metoprolol 200mg Tab PO OD X 30 DaysDocument3 pagesDrug Study: METOPROLOL: Metoprolol 200mg Tab PO OD X 30 Daysbobo gamingNo ratings yet
- Standards of Medical Care in Diabetes - 2022: 10. Cardiovascular Disease and Risk ManagementDocument31 pagesStandards of Medical Care in Diabetes - 2022: 10. Cardiovascular Disease and Risk ManagementAdina SimionNo ratings yet
- Module 3 Diabetes MellitusDocument15 pagesModule 3 Diabetes MellitusNor Jeannah PolaoNo ratings yet
- Practice Guidelines: High Blood Pressure: ACC/AHA Releases Updated GuidelineDocument3 pagesPractice Guidelines: High Blood Pressure: ACC/AHA Releases Updated GuidelineIris N MNo ratings yet
- Case Study 3 - HCVDDocument12 pagesCase Study 3 - HCVDJilkiah Mae Alfoja CampomanesNo ratings yet
- Medip, IJCP-2856 ODocument6 pagesMedip, IJCP-2856 OMarcelita DuwiriNo ratings yet
- Diuretics: Common Diuretics (Thiazides, Loop, K-Retaining)Document1 pageDiuretics: Common Diuretics (Thiazides, Loop, K-Retaining)Andrew AkramNo ratings yet
- Bates Chapter 4 Flashcards - QuizletDocument8 pagesBates Chapter 4 Flashcards - Quizletaznknight323No ratings yet
- Science UnsolDocument31 pagesScience UnsolAmaan KhanNo ratings yet
- Ethnobotanical Study of Acalypha Wilkesiana (Euphorbiaceae), A Plant Used in The Treatment of Arterial Hypertension in Oyem in Northern GabonDocument6 pagesEthnobotanical Study of Acalypha Wilkesiana (Euphorbiaceae), A Plant Used in The Treatment of Arterial Hypertension in Oyem in Northern GabonOpenaccess Research paperNo ratings yet
- Guidelines For HCMDocument2 pagesGuidelines For HCMDhamscen Lopez EscurelNo ratings yet
- 01 Diabetes Mellitus Type2Document39 pages01 Diabetes Mellitus Type2Che HaniffNo ratings yet
- Yang Sheng 0211Document55 pagesYang Sheng 0211Redbaron88No ratings yet
- Referral Letter To Specialist From GPDocument74 pagesReferral Letter To Specialist From GPyazz80% (5)
- Benefits and Drawbacks of Tele MedicineDocument11 pagesBenefits and Drawbacks of Tele MedicinessriraghavNo ratings yet
- College of Nursing: Name: Krizia Mae A. Mendoza Section: BSN 2-1Document9 pagesCollege of Nursing: Name: Krizia Mae A. Mendoza Section: BSN 2-1Nikki Coleen SantinNo ratings yet
- Mind-Body Medicine - University of Maryland Medical CenterDocument17 pagesMind-Body Medicine - University of Maryland Medical Centerjle_dlNo ratings yet
- Chronic Kidney DiseaseDocument283 pagesChronic Kidney DiseaseloisebadNo ratings yet
- FAandDZ PDFDocument8 pagesFAandDZ PDFCosmin GabrielNo ratings yet