You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Clinical Psychology For Trainees 3rd Ed.Document363 pagesClinical Psychology For Trainees 3rd Ed.saeedz2100% (5)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Psychiatric Medication Use in Pregnancy and BreastfeedingDocument19 pagesPsychiatric Medication Use in Pregnancy and BreastfeedingYamiletRomeroVillaNo ratings yet
- UnitedHealthcare Choice Plus 1000Document10 pagesUnitedHealthcare Choice Plus 1000govindhegdeNo ratings yet
- ΠΟΙΟ ΑΝΘΟΙΑΜΑ ΤΑΙΡΙΑΖΕΙ ΣΤΗΝ ΠΕΡΙΠΤΩΣΗ ΜΟΥ?Document25 pagesΠΟΙΟ ΑΝΘΟΙΑΜΑ ΤΑΙΡΙΑΖΕΙ ΣΤΗΝ ΠΕΡΙΠΤΩΣΗ ΜΟΥ?Athina MargatinaNo ratings yet
- Nursing Clinical Rubric PDFDocument5 pagesNursing Clinical Rubric PDFAnonymous iG0DCOf100% (2)
- Region: X Province: Lanao Del Norte City/Municipality: Nunungan Barangay: PanganapanDocument6 pagesRegion: X Province: Lanao Del Norte City/Municipality: Nunungan Barangay: PanganapanAlrafie N. MONARANo ratings yet
- HS 2712 LJ Unit 4Document3 pagesHS 2712 LJ Unit 4Adanigbo MagretNo ratings yet
- JNTU Hyderabad: B.Pharmacy Regular/Supplementary Examinations Time Table 2011-2012Document6 pagesJNTU Hyderabad: B.Pharmacy Regular/Supplementary Examinations Time Table 2011-2012MahabubnagarNo ratings yet
- RHUDocument34 pagesRHULore Anne Mhae SantosNo ratings yet
- Blockchain in Healthcare Sector: A Case Study of NepalDocument12 pagesBlockchain in Healthcare Sector: A Case Study of NepalResma GhimireNo ratings yet
- MiracleDocument11 pagesMiracleJonatasCostaNo ratings yet
- MSF Clinical GuidelinesDocument344 pagesMSF Clinical GuidelinesmargongabNo ratings yet
- Final Evaluation - 2021Document12 pagesFinal Evaluation - 2021api-240864098No ratings yet
- MSF OCA NCD Guidelines v5.2 2020Document143 pagesMSF OCA NCD Guidelines v5.2 2020Md. Rubayet HossainNo ratings yet
- Evaluating The Effectiveness of The "Germ-Free Hands " Intervention For Improving The Hand Hygiene Practices of Public Health StudentsDocument9 pagesEvaluating The Effectiveness of The "Germ-Free Hands " Intervention For Improving The Hand Hygiene Practices of Public Health StudentsnoviaNo ratings yet
- FluconazoleDocument5 pagesFluconazoleGreats HalomoanNo ratings yet
- Client AssessmentDocument4 pagesClient Assessmentapi-488704485No ratings yet
- 17-2-1 CM Regulatory Agencies PPDocument21 pages17-2-1 CM Regulatory Agencies PPAhmed TorkyNo ratings yet
- Annual Accomp - Report - 2021Document4 pagesAnnual Accomp - Report - 2021Amiel GuarinNo ratings yet
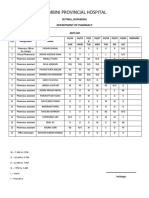
- Lumbini Provincial Hospital: Department of PharmacyDocument2 pagesLumbini Provincial Hospital: Department of PharmacyImdadHussainOPositiveNo ratings yet
- 2022 - European Guideline Dermite AtopiqueDocument23 pages2022 - European Guideline Dermite AtopiqueLydia LydiaNo ratings yet
- Hospital Incident Management TeamDocument23 pagesHospital Incident Management TeamMary Joy GarciaNo ratings yet
- NCM 101 Lecture 1 Intro To Health AssessmentDocument4 pagesNCM 101 Lecture 1 Intro To Health AssessmentRaRe TVNo ratings yet
- Introduction To Translational Science - CourseraDocument4 pagesIntroduction To Translational Science - CourseraSamNo ratings yet
- The Next Generation Nclex - Strategies For Success With Speaker NotesDocument47 pagesThe Next Generation Nclex - Strategies For Success With Speaker Notesapi-308471999No ratings yet
- History of SurgeryDocument22 pagesHistory of SurgeryPrachi KharatmalNo ratings yet
- Health Problems Family Nursing Problems Goal of Care Objectives of Care Intervention Plan Rationale Evaluation Nursing InterventionsDocument4 pagesHealth Problems Family Nursing Problems Goal of Care Objectives of Care Intervention Plan Rationale Evaluation Nursing InterventionsColleen De la RosaNo ratings yet
- New Vision University Syllabus: 1. General InformationDocument11 pagesNew Vision University Syllabus: 1. General InformationkharaNo ratings yet
- Results: Amir Hamdi, Aimaz Afrough, Mahdi Farhoudi, Haleh Hamdi, Ghaffar ShokouhiDocument1 pageResults: Amir Hamdi, Aimaz Afrough, Mahdi Farhoudi, Haleh Hamdi, Ghaffar ShokouhiDanyal SiddiquiNo ratings yet
- Special 510 (K) Summary: Medtronic VascularDocument6 pagesSpecial 510 (K) Summary: Medtronic VascularManoj NarukaNo ratings yet