You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- FREE PRINTABLE CNA Practice ExamDocument12 pagesFREE PRINTABLE CNA Practice Examheartandhandstraining_com91% (57)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- General Format For Orthopedic AssessmentDocument27 pagesGeneral Format For Orthopedic AssessmentMegha Patani100% (7)
- Solution Manual For Fordneys Medical Insurance 15th Edition Linda SmithDocument24 pagesSolution Manual For Fordneys Medical Insurance 15th Edition Linda SmithSarahAlexanderrkcq100% (39)
- Development of Framework For Software SecurityDocument8 pagesDevelopment of Framework For Software SecuritygovindasamyNo ratings yet
- EFA For Components Using FEADocument11 pagesEFA For Components Using FEAgovindasamyNo ratings yet
- Analysis of Maintenance Failure at A Nuclear Power PlantDocument10 pagesAnalysis of Maintenance Failure at A Nuclear Power PlantgovindasamyNo ratings yet
- 1Document8 pages1govindasamyNo ratings yet
- Lakahl IJQRM 2006Document23 pagesLakahl IJQRM 2006govindasamyNo ratings yet
- Criscione Root Cause Analysis v2Document28 pagesCriscione Root Cause Analysis v2JESIN2412No ratings yet
- Iv Infusion Pumps: PurposeDocument4 pagesIv Infusion Pumps: PurposegovindasamyNo ratings yet
- Markov ProcessDocument3 pagesMarkov ProcessgovindasamyNo ratings yet
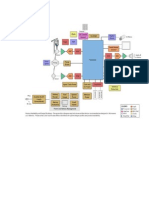
- Block DiagramDocument1 pageBlock DiagramgovindasamyNo ratings yet
- Lung Adenocarcinoma Case PresentationDocument29 pagesLung Adenocarcinoma Case PresentationthekidthatcantNo ratings yet
- Sensus Harian TGL 02 Maret 2022...........Document121 pagesSensus Harian TGL 02 Maret 2022...........Ruhut Putra SinuratNo ratings yet
- Biomedical Equipment Technology Bet1Document1 pageBiomedical Equipment Technology Bet1Rufaida HussainNo ratings yet
- Thesis Statement For Nicotine AddictionDocument8 pagesThesis Statement For Nicotine Addictiongbww46x7100% (2)
- Determinants of HealthDocument29 pagesDeterminants of HealthMayom Mabuong92% (12)
- Infection and Tumorigenesis of Biomaterials by Smit Prajapati-200280103028 and Yukta Dodia - 200280103052Document18 pagesInfection and Tumorigenesis of Biomaterials by Smit Prajapati-200280103028 and Yukta Dodia - 200280103052Yukta DodiaNo ratings yet
- Hospital Statistics Report On 8.5.2020Document4 pagesHospital Statistics Report On 8.5.2020vaideeswari kumarNo ratings yet
- Evidence Based Assessment of OCDDocument17 pagesEvidence Based Assessment of OCDDanitza YhovannaNo ratings yet
- Comparision US UK Japan RegulationsDocument5 pagesComparision US UK Japan RegulationsProschool HyderabadNo ratings yet
- BSN 3-B (GROUP 2) - CLINICAL CASE ANALYSIS - Arthritis (REVISED)Document7 pagesBSN 3-B (GROUP 2) - CLINICAL CASE ANALYSIS - Arthritis (REVISED)Florence Dumawal FariñasNo ratings yet
- A Rural Mental Health CrisisDocument13 pagesA Rural Mental Health CrisisKeri StrahlerNo ratings yet
- PRN Effectiveness PresentationDocument14 pagesPRN Effectiveness Presentationapi-457177638No ratings yet
- Mechanical Therapy: by Nikola TeslaDocument2 pagesMechanical Therapy: by Nikola TeslaRommy RahmansyahNo ratings yet
- PartografDocument31 pagesPartografrovi wilmanNo ratings yet
- Onco-Critical Care An Evidence-Based ApproachDocument539 pagesOnco-Critical Care An Evidence-Based ApproachZuriNo ratings yet
- Parkinson S Disease Epidemiology,.9Document5 pagesParkinson S Disease Epidemiology,.9bacharelado2010No ratings yet
- Status Asthmaticus Case StudyDocument18 pagesStatus Asthmaticus Case Studygeorgeloto12No ratings yet
- Hypernatremia PediatricsDocument7 pagesHypernatremia PediatricsJOHANNESKIFENDINo ratings yet
- Massage Therapy - Basic Techniques of Swedish Massage - Massage - Therapeutic Massage - Swedish MassageDocument1 pageMassage Therapy - Basic Techniques of Swedish Massage - Massage - Therapeutic Massage - Swedish MassagenaveenNo ratings yet
- Allen Part Pedia CaseDocument3 pagesAllen Part Pedia CasePaul Michael Baguhin0% (1)
- Laporan Persediaan 1sd30okt2023Document28 pagesLaporan Persediaan 1sd30okt2023ARIEF YUNIARDINo ratings yet
- Mrs. Manisha Chichani 29032023 064453 PMDocument1 pageMrs. Manisha Chichani 29032023 064453 PMManisha ChichaniNo ratings yet
- Devoir de Synthèse N°2 2011 2012 (Lycée Ali Bourguiba Bembla)Document4 pagesDevoir de Synthèse N°2 2011 2012 (Lycée Ali Bourguiba Bembla)ferchichi halimaNo ratings yet
- Arihant Hospital & Research CentreDocument30 pagesArihant Hospital & Research CentreSourabhSharmaNo ratings yet
- Sitecore - Media Library - Files.3d Imaging - Shared.7701 3dbrochure UsDocument28 pagesSitecore - Media Library - Files.3d Imaging - Shared.7701 3dbrochure UsandiNo ratings yet
- 7 Essential Steps of CPRDocument2 pages7 Essential Steps of CPRBea YmsnNo ratings yet
- Health FormsDocument5 pagesHealth FormsBianca Louise SengcoNo ratings yet