IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 14, Issue 10 Ver. XI (Oct. 2015), PP 55-60
www.iosrjournals.org
Deceased Donor Renal Transplantation: A South Indian
Experience.
Periasamy Ponnusamy1, Thiruvarul Palanisamy Venkatachalam2,
Pitchaibalashanmugam Karuppaiah3,Kulthe Ramesh Seetharam Bhat4
1, 2, 3, 4
(Department of urology, Govt Stanley medical College, India)
Abstract: The first deceased donor kidney transplant in our hospital was performed in 1996 with74deceased
donor transplantations thereafter.We retrospectively analysed various donor and recipient characteristics with
focus on vessel anatomy and type of anastomosis. Intraoperative andpost-operativecomplications. Patient and
graft survival rates of deceased donor renal transplant recipientsat 1 year & 3 years.Donor age was between1268 years. Main cause of brain death was RTA.Recipientage was between 18-57years. Only19(25.67%)
werefemales. Etiology for ESRD was not known in many, followed by CGD. Average Cold ischemia time was
8.01 ( 2.73) hours.17 (22.97%) cadaveric kidney had double renal arteriesof which, in 10 accessoryarteries
were ligated, double anastomosis to External Iliac arteryand Internal iliac artery was done in others.
Intraoperative one case eachof mottling and impending graft rupture was encountered. Postoperatively
23(31.5%)cases had DGF and 5(6.8%) had SGF. 11(14.86%) patients developed sepsis, 7(9.5%) had
pneumonitis, one case each of graft artery thrombosis and anastomotic dehiscence seen.1 year Survival rates
was 89.33 % and 73 % for patient and graft respectively.3 year survival rate was56.4 % and 44% for patient
and graft respectively.
Keywords: Deceased donor renal transplantation, graft vascular anomalies, cold ischaemic times.
I.
Introduction
In India the End Stage Renal Disease (ESRD) is a major disease burden 1 .Crude incidence rates of - 151
per million population per year 1 and the age- adjusted incidence rates is around 232 per million population per
year.1The renal transplantation rates are only 3.20 per million populations per year. 1 Of which 2% of total
kidneys procured from deceased renal donor. 2
The state of Tamilnadu has been a pioneer in deceased donor renal transplantation with good political
will and commitment a successful program has been running in the state for nearly 15 years now. We have
published our data incorporating our challenges we faced and our results.
II.
Aims
To analyse various donor and recipient characteristics with focus on vessel anatomy and type of
anastomosis.
To analyse Intraoperative and post-operative complications
To analyse Patient and graft survival rates of deceased donor renal transplant recipients
III.
Methodology
We did a Retrospective analysis of all cadaver transplant from October 2008 to July 2014. The donor recipient characteristics, post-transplant complication and graft function were analysed. Kaplan-Meier analysis
to evaluate survival rates of patient & graft at 1 year & 3 years. Total number of deceased donor transplantation
studied was 74 (n)
IV.
Results
Donor characteristics
It is our department policy not to refuse any graft. Multiple vessel grafts have also been used. Only one
graft refused out of total where there was a hilar rent in the vein. The age of donor was between 12-68 years.The
mean age of donor was 33.51 ( 13.3) years
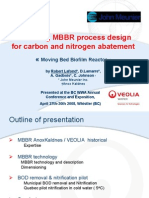
Main cause of brain death was RTA with almost 57 grafts from this category. 13 had fall from height with 1
deceased donor had fall at home, 2 aneurysmal bleed and 1 had traumatic asphyxia. 3 fit into extended criteria
for deceased donors who were either hypertensive or Sr. creatinine more than 1.5 g/dl. Most of the grafts were
from right side, totally 44 in number.
DOI: 10.9790/0853-1410115560
www.iosrjournals.org
55 | Page
Deceased Donor Renal Transplantation: A South Indian Experience.
2 11
13(
17.56%)
57(77.0
2%)
RTA
FALL FROM HT
ANEURYSMAL BLEED
SAH
TRAUMATIC ASPHYXIA
Fig no 1- Pie chart showing causes of deceased donor deaths
Table No. 1 showing Frequency of the side of graft.
Side of graft
Right
Left
Total
Frequency
44
30
74
Percent
59.45
40.54
100.0
Recipient characteristics
The Recipient age was between 18-57 years.The overall mean of recipient was 34 ( 7.8) years.
19(25.67%) were females.Etiology for ESRD was not known in 38 recipients and 27 had chronic
glomerulonephritis. The mean duration of dialysis in our recipient group was 20.1 months with minimum of 1
month and maximum of 60 months on dialysis.
2
3
NOT KNOWN
11
2
27 ( 36.48%)
38(51.3
5%)
CGN
ADPKD
FSGS
ALPORTS
IgAN
SLE
Fig no 2:- Pie chart showing Etiology of CKD in recipients.
Graft vascular anatomy
In our series, 17 of our grafts had double renal artery. Out of which upper polar accessory artery ligated
in 10 patients.Double anastomosis to EIA and IIA was done in 7 patients.
6 of our patients had triple renal arteries. ALL in SINGLE CUFF ANASTOMOSIS was done in 4
patients. Two in cuff and one single artery anastomosis done in 1patients (with one vessel anastomosed end to
end). Three individual anastomosis was done in 1 patient. One patient had double renal vein.9 patients with
vascular anomalies had delay graft function and rest had normal graft functions.
Cold ischemic times
In our series the mean Cold Ischemic times was 8.01 ( 2.73) hours in deceased donor renal
transplantation, with minimum CIT of 3 hours when graft was harvested from our centre and maximum time of
DOI: 10.9790/0853-1410115560
www.iosrjournals.org
56 | Page
Deceased Donor Renal Transplantation: A South Indian Experience.
15 hours when the graft was harvested from other centres. It was noted that there was no difference in graft
function among groups with CIT less than 8 hours and with CIT beyond 12 hours.
Table no 2:- showing comparison of graft outcome with cold ischemic times
Cold ischemia time
Upto 8 hours
8-10 hours
Beyond 10 hours
DGF/SGF
12( 32)
4(18)
12(24)
Graft preservation
HTK (Histidine-Tryptophan-Alpha Ketoglutarate) CUSTODIOL was used in all the deceased donor
transplantations. Thestandard sterile three bag technique is used for packing and transportation is done in sterile
ice.
Cost of HTK is a major limitation
Induction agent
Anti-Thymocyte Globulin rabbit origin (rATG). A single dose of 1.5 mg/kg was given as intravenous
infusion in the preoperative and intraoperative period. Valganciclovir 450 mg twice daily is given for three
months for Cytomegalovirus prophylaxis if ATG is used
Other induction agent used was Interleukin-2 receptor blockers (Basiliximab) which is given as two
doses of 20 mg each is given at 4 days interval. First just before surgery followed by second dose 4 days later.
Routine post-operative care protocol included
Input/ output charting
Renal function test
Immunosuppression
Tacrolimus
Mycophenolate mofetil
Predinisolone.
Doppler ultrasound when necessary.
Renal biopsy rarely
Tacrolimus levels at day 4 and day 10
Table no 3:- Frequency of Intraoperative events
INTRA OP EVENTS
Absent
Present
Total
Frequency
66
8
74
Percent
89.18
10.82
100.0
Among the cases of that had intraoperative events included mottling in one, impending graft rupture in
one, bleeding in two and hypotension in four cases.
Table no 4:- Frequency of Post-operative events:POST OP EVENTS
Absent
Present
Total
Frequency
44
30
74
Percent
58.9
41.1
100.0
11(14.86%) patients developed sepsis in the post-operative period, 7(9.5%) patient had pneumonitis, 9
patients had persistent drain, 2 patients had pancreatitis and one patient had right lower limb ischemia following
external iliac artery thrombosis.
DOI: 10.9790/0853-1410115560
www.iosrjournals.org
57 | Page
Deceased Donor Renal Transplantation: A South Indian Experience.
Table no 5:-Post operative graft function outcomes
GRAFT FUNCTION
Frequency
Percent
Normal
46
62.16
DGF
23
31.08
SGF
6.75
Total
74
100.0
23(31.5%) cases had DGF and5(6.8%) had SGF in the immediate post-operative period.Rest had
normal graft function.
4 patients had nephrectomies. Two cases intraoperatively that had mottling and impending graft rupture
were removedand two cases with graft artery thrombosis and anastomotic site dehiscence respectively were
removed in the post-transplant period.
Other post-operative parameters
The mean follow up period was 3 years.The meanpost-operative urine output was 6733.33 ml on day 1.
The mean baseline serum creatinine was 1.45 (0.42) mg/dl on follow up. New onset of Diabetes after renal
transplant (NODAT) was observed in 10(13.69 %) patients. The mean tacrolimus levels on fourth postoperative
day were: 6.75 (4.05) ng/ml.Acute cellular rejections were encountered in 7 (9.58 %) patients. Acute antibody
mediated rejection was encountered in 2 (2.74%) patients. Biopsy proven acute tubular necrosis (ATN) was
observed in 6 (8.21 %) patients.
In the follow up period 10 patients developed sepsis with no identifiable focus of infection. 7 patient
had Pneumonitis of various aetiologies.Recurrent UTI and BK virus was seen in 1 each. 1 patient had HCV
Related DCLD. 6 of our patients had mycobacterial infections. Mycobacterial tuberculous infections were seen
in 6 patients.4 patients had lymph nodal involvement and 2 patients had pulmonary tuberculosis.
Survival rates
1 yr. survival rates was 89.33 % for patients and 73% for graft respectively.
At 3 year survival rate for Patient was 56.4 % and for graft was 44% respectively.
Survival Function
1.0
Cum Survival
.8
.6
.4
.2
Survival Function
0.0
Censored
0
500
1000
1500
2000
No of days alive
Fig No: - 3 Kaplan Meier analysis of patient survival
DOI: 10.9790/0853-1410115560
www.iosrjournals.org
58 | Page
Deceased Donor Renal Transplantation: A South Indian Experience.
Survival Function
1.2
1.0
Cum Survival
.8
.6
.4
.2
Surviva l Function
0.0
Censor ed
0
500
1000
1500
2000
No of days graft functioned
Fig No 4 Kaplan Meier analysis of graft survival
V.
Discussion
The deceased donor renal transplantation in our country is still in its infancy. While the rates of
deceased donor renal transplantation in US and Europe are high, it has not materialized in many states in India.
We present a series of deceased donor renal transplantation done at our institution from 2008 to 2012. A unique
fact about our Centre is that it caters to the patients of poor socio economic strata who live in substandard living
conditions. The source of kidney was predominantly from victims of road traffic accidents as usually these are
young people with no comorbidities and the graft was usually from right side as most of the time the source of
the graft is from other centre.
There are many factors that determine the immediate graft function which include Risk factors for DGF
in cadaver renal transplantation are Donor age (>50 years),Cold ischemia time (>12 hrs.),Recipient race ,Panel
Reactive Antibodies (>50%), HLA mismatch, graft vascular anatomy and duration of dialysis.1,2In our series,
the mean donor age was well below 50 years except in 4 cases and all recipients were of same race, Panel
Reactive antibodies less than 50 and HLA cross match of less than 5-10 %.
The overall outcomes of deceased donor transplantation in our series is compared with other series below
Table No 6:- Comparison of patient and graft outcomes in different studies
Patient
1 Year (%)
Takashi.M. et al (n= 56) 3
Shroff et al
( n=100)4
Mani et al 5
Gumber M.R. et al
( n=160) 6
Swami Y.K et al (n= 35) 8
Our data
( n= 74)
86
79.58(1 yr.)
83.8
89.33
Patient
( Year) (%)
96.52 (15 yrs.)
80 (2 yrs.)
76.7(2 yrs.)/
74.8(3 yrs.)
61.2(3 yrs.)
56.44(3 yrs.)
Graft
1 year (%)
89
82
72
92.4
Graft ( Year)
(%)
80.3 (5yrs.)
74 (2 yrs.)
63(4yrs.)
87.9 (2 and 3 yrs.)
95.4
73
79.3(3 Yrs.)
44
(3 yrs.)
In this paper we have mainly discussed the impact of cold ischemic times and graft vascular anatomy
outcomes. The table below gives a comparison of graft outcomes with cold ischemic times.
Table no 7:- Comparison of cold ischemic times with delayed graft function.
Moyers.C et al 8
Swami Y K et al 7
Gumber M R et al 6
Mehta T R et al 9
Our data
Cold ischemic times
( hours)
15
6.25 +/- 2.5
5.56 +/- 2.04
10.3 +/- 4( inter-city)
4.2+/- 1.8( Ahmedabad)
8.01+/-2.73
Delayed graft function (%)
20.8 (machine perfused)
26.5 ( cold preservation)
34
30.6
42.4
22.2
31.5
Our series had comparable graft function with other series in India whereas Moyers.C had reported a
better graft outcomes in spite of having higher cold ischemic times.8 This probably could be due to postoperative factors like higher dose of immunosuppression given in western countries which our nephrologist here
DOI: 10.9790/0853-1410115560
www.iosrjournals.org
59 | Page
Deceased Donor Renal Transplantation: A South Indian Experience.
find it difficult to give due to fear of infections. As per table a subgroup analysis was done in our series and the
outcome did not vary if cold ischemic times were below or above 10 hours (TABLE NO-3).
The use of grafts with multiple renal arteries has been considered a relative contraindication because of
the increased incidence of vascular and urologic complication. 17 cases had doublerenal artery and in many the
upper polar artery was sacrificed, however we were careful with 6 cases with triple vessels where we feel it is
mandatory to preserve all vessels as the vessels are of equal caliber and have equal perfusion.10, 11, 12, 13
In our series we had good graft function in up to 1 year in comparison with other series however our
graft outcomes and patient outcome were inferior at the end of 3 years. Of 74 patients 28 patients died. There
are many reasons for this of which infection were a major culprit. We had almost more than a 3 rd of patients
with infective complication leading to graft failure and subsequently for poor patient survival. Second important
reason is more rejection rates as our tendency is to give reduced doses of immunosuppressive drugs due to fear
of infection. The infection rates are probably higher due to poor socioeconomic status of our patient groups and
poor hygiene and sanitary condition of our patients.
With the adequate counselling we have been able to educate patient about basic sanitation but it is
difficult for them to maintain same due to poverty and also their neighbors and friends fail to do so leading to
inevitable exposure to infective agents.
Though the transplant procedure in the state of Tamilnadu is funded by the government through chief
ministers insurance scheme, which is a boon to the people of low socioeconomic strata it is however difficult to
withstand cost incurred in thepost-transplant period. In spite of free medications offered by the government the
cost incurred in travel, recurrent hospitalization, cost of relatives stay around our institute and their food
expenses in case of hospitalization are high.
VI.
Conclusion
Deceased donor renal transplantation is way to increase graft pool with prolonged cold ischemic times
and multiple renal arteries is not a deterrent to transplant, however it is essential to promote a positive public
attitude, identification of early brain death and certification, getting prompt consent for organ donation, develop
adequate hospital infrastructure and cover long term cost post transplantation in poor patients. Cadaver organs
should be considered as nations resource and organs wasted should be treated as lives lost.
Acknowledgement
The authors acknowledge the encouragement and support offered by the Dean - Dr.Isaac Christian
Moses, head of the department of urology-Prof.Dr.P. Govindarajan and head of the department of nephrologyDr. Edwin Fernandoin preparing this paper.
References
[1].
[2].
[3].
[4].
[5].
[6].
[7].
[8].
[9].
[10].
[11].
[12].
[13].
Jha.V .Current status of end-stage renal disease care in India and Pakistan, Kidney International Supplements (2013) 3, 157160;
doi:10.1038/kisup.2013.3
Shroff S. Indian transplant registry. Indian J Urol 2007;23:272-7.
Tasaki, M. et al.20-Year Analysis of Kidney Transplantation: A Single Center; Japan Transplantation Proceedings , Volume 46 ,
Issue 2 , 437 - 441
Shroff S, Navin S, Abraham G, Rajan PS, Suresh S, Rao S, et al. Cadaver organ donation and transplantation-an Indian perspective.
Transplant Proc 2003;35:15-7.
Mani MK. Review article, development of cadaver renal transplantation in India. Nephrology 2002;7:177-82.
Gumber M R, Kute V B, Goplani K R, Shah P R, Patel H V, Vanikar A V, Modi P R, Trivedi H L. Deceased donor organ
transplantation: A single center experience. Indian J Nephrol [serial online] 2011 [cited 2015 Jan 26];21:182-5. Available
from: http://www.indianjnephrol.org/text.asp?2011/21/3/182/82636
Swami YK, Singh DV, Gupta SK, Pradhan AA, Rana YP, Harkar S, Wani M S. Deceased donor renal transplantation at army
hospital research and referral: Our experience. Indian J Urol 2013;29:105-9
Moyers et al. Machine Perfusion or Cold Storage in Deceased-Donor Kidney Transplantation.N Engl J Med 2009; 360:7-19January
1, 2009DOI: 10.1056/NEJMoa0802289
Mehta T R, Shah V R, Butala B P, Parikh G P, Parikh B K, Vora K S, Modi M P, Bhosale G P, Kadam P G, Shah P R, Gumber M
R, Patel H V, Kute V B, Modi P R, Rizvi S J, Vanikar A V, Trivedi H L. Intercity deceased donor renal transplantation: A singlecenter experience from a developing country. Saudi J Kidney Dis Transpl 2013;24:1280-4
Roza AM, Perloff LJ, Naji A, Grossman RA, Barker CF. Living-related donors with bilateral multiple renal arteries. A twenty-year
experience. Transplantation. 1989;47:3979. [PubMed]
Oesterwitz H, Strobelt D. Extracorporeal microsurgical repair of injured multiple donor kidney arteries prior to cadaveric
allotransplantation. Eur Urol. 1985;11:100105. [PubMed]
Makiyama K, Tanabe K, Ishida H, Tokumoto T, Shimmura H, Omoto K, Toma H. Successful renovascular reconstruction for renal
allografts with multiple renal arteries.Transplantation.2003;75:828832.doi: 10.1097/01.TP.0000054461.57565.18. [PubMed]
[Cross Ref]
Ali-El-Dein B, Osman Y, Shokeir AA, Shehab El-Dein AB, Sheashaa H, Ghoneim MA. Multiple arteries in live donor renal
transplantation: surgical aspects and outcomes. J Urol. 2003;169:20137. [PubMed]
DOI: 10.9790/0853-1410115560
www.iosrjournals.org
60 | Page
You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Kimberly Callis - Stoning Demons - Complex PTSD Recovery Workbook. 6Document44 pagesKimberly Callis - Stoning Demons - Complex PTSD Recovery Workbook. 6intenselight91% (11)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Kinesics, Haptics and Proxemics: Aspects of Non - Verbal CommunicationDocument6 pagesKinesics, Haptics and Proxemics: Aspects of Non - Verbal CommunicationInternational Organization of Scientific Research (IOSR)No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Adjuvant Analgesics (2015) PDFDocument177 pagesAdjuvant Analgesics (2015) PDFsatriomega100% (1)
- Rehab-U FreeMobilityEbook PDFDocument10 pagesRehab-U FreeMobilityEbook PDFTuteraipuni POTHIERNo ratings yet
- Types of PsychologyDocument62 pagesTypes of PsychologyParamjit SharmaNo ratings yet
- Coding Handbook - Doc 6-16-09 Revised 8 14 09 AddDocument52 pagesCoding Handbook - Doc 6-16-09 Revised 8 14 09 AddcindybevNo ratings yet
- High Yield Step 2ckDocument4 pagesHigh Yield Step 2ckCesar_Palana_3832No ratings yet
- Human Rights and Dalits: Different Strands in The DiscourseDocument5 pagesHuman Rights and Dalits: Different Strands in The DiscourseInternational Organization of Scientific Research (IOSR)No ratings yet
- Case Study Celiac DiseaseDocument8 pagesCase Study Celiac Diseaseapi-242376719No ratings yet
- Nutrition Questionnaire-Focused PregnancyDocument2 pagesNutrition Questionnaire-Focused PregnancyJing Cruz100% (1)
- Dysfunctional Gastrointestinal Motility Maybe Related To Sedentary Lifestyle and Limited Water Intake As Evidenced byDocument6 pagesDysfunctional Gastrointestinal Motility Maybe Related To Sedentary Lifestyle and Limited Water Intake As Evidenced byCecil MonteroNo ratings yet
- Bronchial Asthma Nursing Care PlansDocument2 pagesBronchial Asthma Nursing Care PlansdeincediannaNo ratings yet
- Chron's Disease 2Document3 pagesChron's Disease 2TarantadoNo ratings yet
- Liceo de Cagayan University: Acute AppendicitisDocument2 pagesLiceo de Cagayan University: Acute AppendicitisKylie AstrudNo ratings yet
- Fu Zhen and TurtleDocument7 pagesFu Zhen and Turtledrakpo100% (2)
- 2 05MasteringMBBRprocessdesignforcarbonandnitrogenabatementDocument65 pages2 05MasteringMBBRprocessdesignforcarbonandnitrogenabatementYên BìnhNo ratings yet
- The Impact of Technologies On Society: A ReviewDocument5 pagesThe Impact of Technologies On Society: A ReviewInternational Organization of Scientific Research (IOSR)100% (1)
- OLFU Intesive Post Test 50 ItemsDocument5 pagesOLFU Intesive Post Test 50 ItemsmonmonNo ratings yet
- Asthma in PregnancyDocument40 pagesAsthma in PregnancyKabo75% (4)
- Socio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanDocument7 pagesSocio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanInternational Organization of Scientific Research (IOSR)No ratings yet
- "I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweDocument5 pages"I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweInternational Organization of Scientific Research (IOSR)No ratings yet
- Assessment of The Implementation of Federal Character in Nigeria.Document5 pagesAssessment of The Implementation of Federal Character in Nigeria.International Organization of Scientific Research (IOSR)No ratings yet
- An Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyDocument14 pagesAn Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyInternational Organization of Scientific Research (IOSR)No ratings yet
- A Review of Rural Local Government System in Zimbabwe From 1980 To 2014Document15 pagesA Review of Rural Local Government System in Zimbabwe From 1980 To 2014International Organization of Scientific Research (IOSR)No ratings yet
- Relationship Between Social Support and Self-Esteem of Adolescent GirlsDocument5 pagesRelationship Between Social Support and Self-Esteem of Adolescent GirlsInternational Organization of Scientific Research (IOSR)No ratings yet
- A Proposed Framework On Working With Parents of Children With Special Needs in SingaporeDocument7 pagesA Proposed Framework On Working With Parents of Children With Special Needs in SingaporeInternational Organization of Scientific Research (IOSR)No ratings yet
- Attitude and Perceptions of University Students in Zimbabwe Towards HomosexualityDocument5 pagesAttitude and Perceptions of University Students in Zimbabwe Towards HomosexualityInternational Organization of Scientific Research (IOSR)No ratings yet
- The Role of Extrovert and Introvert Personality in Second Language AcquisitionDocument6 pagesThe Role of Extrovert and Introvert Personality in Second Language AcquisitionInternational Organization of Scientific Research (IOSR)No ratings yet
- Comparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesDocument7 pagesComparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesInternational Organization of Scientific Research (IOSR)No ratings yet
- Investigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehDocument4 pagesInvestigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehInternational Organization of Scientific Research (IOSR)No ratings yet
- Importance of Mass Media in Communicating Health Messages: An AnalysisDocument6 pagesImportance of Mass Media in Communicating Health Messages: An AnalysisInternational Organization of Scientific Research (IOSR)No ratings yet
- Edward Albee and His Mother Characters: An Analysis of Selected PlaysDocument5 pagesEdward Albee and His Mother Characters: An Analysis of Selected PlaysInternational Organization of Scientific Research (IOSR)No ratings yet
- The Lute Against Doping in SportDocument5 pagesThe Lute Against Doping in SportInternational Organization of Scientific Research (IOSR)No ratings yet
- Beowulf: A Folktale and History of Anglo-Saxon Life and CivilizationDocument3 pagesBeowulf: A Folktale and History of Anglo-Saxon Life and CivilizationInternational Organization of Scientific Research (IOSR)No ratings yet
- Topic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshDocument7 pagesTopic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshInternational Organization of Scientific Research (IOSR)No ratings yet
- Role of Madarsa Education in Empowerment of Muslims in IndiaDocument6 pagesRole of Madarsa Education in Empowerment of Muslims in IndiaInternational Organization of Scientific Research (IOSR)No ratings yet
- Classical Malay's Anthropomorphemic Metaphors in Essay of Hikajat AbdullahDocument9 pagesClassical Malay's Anthropomorphemic Metaphors in Essay of Hikajat AbdullahInternational Organization of Scientific Research (IOSR)No ratings yet
- An Exploration On The Relationship Among Learners' Autonomy, Language Learning Strategies and Big-Five Personality TraitsDocument6 pagesAn Exploration On The Relationship Among Learners' Autonomy, Language Learning Strategies and Big-Five Personality TraitsInternational Organization of Scientific Research (IOSR)No ratings yet
- Transforming People's Livelihoods Through Land Reform in A1 Resettlement Areas in Goromonzi District in ZimbabweDocument9 pagesTransforming People's Livelihoods Through Land Reform in A1 Resettlement Areas in Goromonzi District in ZimbabweInternational Organization of Scientific Research (IOSR)No ratings yet
- Women Empowerment Through Open and Distance Learning in ZimbabweDocument8 pagesWomen Empowerment Through Open and Distance Learning in ZimbabweInternational Organization of Scientific Research (IOSR)No ratings yet
- Motivational Factors Influencing Littering in Harare's Central Business District (CBD), ZimbabweDocument8 pagesMotivational Factors Influencing Littering in Harare's Central Business District (CBD), ZimbabweInternational Organization of Scientific Research (IOSR)No ratings yet
- Design Management, A Business Tools' Package of Corporate Organizations: Bangladesh ContextDocument6 pagesDesign Management, A Business Tools' Package of Corporate Organizations: Bangladesh ContextInternational Organization of Scientific Research (IOSR)No ratings yet
- Substance Use and Abuse Among Offenders Under Probation Supervision in Limuru Probation Station, KenyaDocument11 pagesSubstance Use and Abuse Among Offenders Under Probation Supervision in Limuru Probation Station, KenyaInternational Organization of Scientific Research (IOSR)No ratings yet
- Designing of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesDocument5 pagesDesigning of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesIOSRjournalNo ratings yet
- Micro Finance and Women - A Case Study of Villages Around Alibaug, District-Raigad, Maharashtra, IndiaDocument3 pagesMicro Finance and Women - A Case Study of Villages Around Alibaug, District-Raigad, Maharashtra, IndiaInternational Organization of Scientific Research (IOSR)No ratings yet
- A Study On The Television Programmes Popularity Among Chennai Urban WomenDocument7 pagesA Study On The Television Programmes Popularity Among Chennai Urban WomenInternational Organization of Scientific Research (IOSR)No ratings yet
- Euro J of Neurology - 2021 - Van Den Bergh - European Academy of Neurology Peripheral Nerve Society Guideline On DiagnosisDocument28 pagesEuro J of Neurology - 2021 - Van Den Bergh - European Academy of Neurology Peripheral Nerve Society Guideline On DiagnosisSusana RocheNo ratings yet
- Thoughts Thoughts: 'Universe, Please Help Me Maintain An Effective Meditative-State. Thank You.'Document4 pagesThoughts Thoughts: 'Universe, Please Help Me Maintain An Effective Meditative-State. Thank You.'Mincheol KangNo ratings yet
- Cytokines - IntroductionDocument2 pagesCytokines - IntroductionTra gicNo ratings yet
- Motion SicknessDocument5 pagesMotion SicknessIbrahim AbdullahNo ratings yet
- Burning Mouth Syndrome Causes, Symptoms and Treatment (BMSDocument23 pagesBurning Mouth Syndrome Causes, Symptoms and Treatment (BMSmuhammadNo ratings yet
- Stabilisation and Safe Transport of The Critically Ill ChildDocument9 pagesStabilisation and Safe Transport of The Critically Ill ChildAdrian CraciunNo ratings yet
- Biosimilar Insulin GlargineDocument59 pagesBiosimilar Insulin GlarginenellizulfiaNo ratings yet
- Nucleus DropDocument1 pageNucleus DropYovinus DenyNo ratings yet
- Q-MED ADRENALINE INJECTION 1 MG - 1 ML PDFDocument2 pagesQ-MED ADRENALINE INJECTION 1 MG - 1 ML PDFchannalingeshaNo ratings yet
- 4 Daftar PustakaDocument3 pages4 Daftar PustakaDian ApriyaniNo ratings yet
- Medium Opening Activator: (Removable Functional Appliance)Document22 pagesMedium Opening Activator: (Removable Functional Appliance)Abiha AliNo ratings yet
- Gram08 28Document21 pagesGram08 28Hendra Wana Nur'aminNo ratings yet
- A Case Study For Electrical StimulationDocument3 pagesA Case Study For Electrical StimulationFaisal QureshiNo ratings yet
- On The Medicinal Chemistry of Gold Complexes As Anticancer DrugsDocument12 pagesOn The Medicinal Chemistry of Gold Complexes As Anticancer DrugsJeffersonNo ratings yet