You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Acute AbdDocument35 pagesAcute AbdloutheluckyNo ratings yet
- Louis Carrillo NarrativeDocument6 pagesLouis Carrillo NarrativeloutheluckyNo ratings yet
- Outine IdeasDocument3 pagesOutine IdeasloutheluckyNo ratings yet
- Project Pipeline: Reaching Youth in Miami Gardens Through An Interactive STEMM (Science, Technology, Engineering, Math, Medicine) ProgramDocument11 pagesProject Pipeline: Reaching Youth in Miami Gardens Through An Interactive STEMM (Science, Technology, Engineering, Math, Medicine) ProgramloutheluckyNo ratings yet
- Louis Peds PreziDocument30 pagesLouis Peds PreziloutheluckyNo ratings yet
- Congenital Heart Defects Email InfoDocument3 pagesCongenital Heart Defects Email InfoloutheluckyNo ratings yet
- ImmunologyDocument11 pagesImmunologyloutheluckyNo ratings yet
- Lecture 1Document3 pagesLecture 1loutheluckyNo ratings yet
- Eb HPDocument2 pagesEb HPloutheluckyNo ratings yet
- Lecture 2Document3 pagesLecture 2loutheluckyNo ratings yet
- BiochemDocument12 pagesBiochemloutheluckyNo ratings yet
- Lecture 3Document3 pagesLecture 3loutheluckyNo ratings yet
- TB PresentationDocument48 pagesTB PresentationloutheluckyNo ratings yet
- Disease and TreatDocument3 pagesDisease and TreatloutheluckyNo ratings yet
- Louis Peds PreziDocument30 pagesLouis Peds PreziloutheluckyNo ratings yet
- NG SoapDocument2 pagesNG SoaploutheluckyNo ratings yet
- Usually Columnar To SquamousDocument4 pagesUsually Columnar To SquamousloutheluckyNo ratings yet
- Obesity: Louis Carrillo Family Medicine Rotation 3Document33 pagesObesity: Louis Carrillo Family Medicine Rotation 3loutheluckyNo ratings yet
- GSD and LSD Osler FridayDocument20 pagesGSD and LSD Osler FridayloutheluckyNo ratings yet
- Surgery Shelf NotesDocument6 pagesSurgery Shelf Noteslouthelucky0% (1)
- Surgery Shelf NotesDocument6 pagesSurgery Shelf Noteslouthelucky0% (1)
- Test 3Document25 pagesTest 3loutheluckyNo ratings yet
- Path 4Document3 pagesPath 4loutheluckyNo ratings yet
- Path 3Document2 pagesPath 3loutheluckyNo ratings yet
- Neuro NotesDocument7 pagesNeuro NotesloutheluckyNo ratings yet
- Test 3Document28 pagesTest 3loutheluckyNo ratings yet
- Compartment Syndrome Causes and TreatmentDocument8 pagesCompartment Syndrome Causes and TreatmentloutheluckyNo ratings yet
- Test 2Document17 pagesTest 2loutheluckyNo ratings yet
- CeliacDocument1 pageCeliacloutheluckyNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Erin Lanni Resume GradDocument3 pagesErin Lanni Resume Gradapi-242800329No ratings yet
- SCHA SC Healthcare Heroes Truck Map 2020Document14 pagesSCHA SC Healthcare Heroes Truck Map 2020WIS NewsNo ratings yet
- RBM Business Plan (2009 - 2010)Document55 pagesRBM Business Plan (2009 - 2010)Amanze Donatus Uche100% (1)
- M73 Osbo1023 01 Se CH73Document10 pagesM73 Osbo1023 01 Se CH73prexiebubblesNo ratings yet
- Bench MarkingDocument213 pagesBench MarkingManuel Adalid GameroNo ratings yet
- Pharmacoeconomics: Dr. Salim Sheikh Dept. of Pharmacology, VMMC & Safdarjung HospitalDocument80 pagesPharmacoeconomics: Dr. Salim Sheikh Dept. of Pharmacology, VMMC & Safdarjung HospitalSima JabbariNo ratings yet
- 2020-2022 Cdp-2020-2022-List-Of-ProgramsDocument13 pages2020-2022 Cdp-2020-2022-List-Of-ProgramsAira TyNo ratings yet
- InformationBulletin PDFDocument91 pagesInformationBulletin PDFNixon GoyalNo ratings yet
- Master Obat FarmasiDocument75 pagesMaster Obat FarmasiSiska PrasenjaNo ratings yet
- Superficial Vein Thrombosis - 29aug2020Document5 pagesSuperficial Vein Thrombosis - 29aug2020Luis octavio carranzaNo ratings yet
- CDI 5 Prelim ExamDocument2 pagesCDI 5 Prelim ExamRovi ClaritoNo ratings yet
- Mental Health-Process Recording EvaluationDocument7 pagesMental Health-Process Recording EvaluationLeAnna91% (57)
- ACC/AHA Versus ESC/ESH On Hypertension Guidelines: JACC Guideline ComparisonDocument9 pagesACC/AHA Versus ESC/ESH On Hypertension Guidelines: JACC Guideline ComparisonCamila ZorrillaNo ratings yet
- Reproductive Health Strategic Plan 2007-2011Document109 pagesReproductive Health Strategic Plan 2007-2011Nana Adwoa Animah100% (2)
- Liver Abscess ThesisDocument7 pagesLiver Abscess Thesisjenniferalexanderfortlauderdale100% (1)
- Research Paper On India Vision 2020Document10 pagesResearch Paper On India Vision 2020Gopi Khunt100% (1)
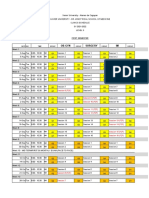
- Level 3 Clinics Schedule Clinics Groupings Group Leaders and PreceptorsDocument24 pagesLevel 3 Clinics Schedule Clinics Groupings Group Leaders and PreceptorsKIM LORIE YAP PASCUALNo ratings yet
- EBN - Asking The ClinicAL QUESTION 2019Document40 pagesEBN - Asking The ClinicAL QUESTION 2019rnrmmanphdNo ratings yet
- The Procedure Note - Laceration RepairDocument2 pagesThe Procedure Note - Laceration RepairDaisy MugaNo ratings yet
- DST Project ProposalDocument2 pagesDST Project ProposalNaveenaAnithaNo ratings yet
- Clinical Lab and Intro To PhleboDocument45 pagesClinical Lab and Intro To PhleboKeren Nathaniel AlvaradoNo ratings yet
- Shortliffe (1987) - Computer Programs To Support Clinical Decision Making PDFDocument6 pagesShortliffe (1987) - Computer Programs To Support Clinical Decision Making PDFKalil MerconhotoNo ratings yet
- Nursing Simulation - Patient EvaluationDocument3 pagesNursing Simulation - Patient EvaluationAaronNo ratings yet
- Detoxification and Toxicology PDFDocument26 pagesDetoxification and Toxicology PDFMetcher Maa AkhiNo ratings yet
- Health10 Q1 L1Document12 pagesHealth10 Q1 L1Jan Den Saul DalanNo ratings yet
- IR - PERPUSTAAN UNIVERSITAS AIRLANGGADocument6 pagesIR - PERPUSTAAN UNIVERSITAS AIRLANGGAYuari AdeNo ratings yet
- Guidelines For The Design and Construction of Health Care FacilitiesDocument370 pagesGuidelines For The Design and Construction of Health Care FacilitiesJay MenaNo ratings yet
- Generating Hope For A Brighter Future: Bringing Electricity To Arua, UgandaDocument36 pagesGenerating Hope For A Brighter Future: Bringing Electricity To Arua, UgandasedianpoNo ratings yet
- The key terms slide defines determinant as "factor that contributes to the generation of a traitDocument68 pagesThe key terms slide defines determinant as "factor that contributes to the generation of a traitOwusu AmosNo ratings yet
- National Policy of Palliative Care in Indonesia - En.idDocument31 pagesNational Policy of Palliative Care in Indonesia - En.idaya PermatasariNo ratings yet