You might also like
- NICARDIPINE HYDROCHLORIDE - Nicardipine Hydrochloride CapsuleDocument8 pagesNICARDIPINE HYDROCHLORIDE - Nicardipine Hydrochloride CapsulecynthiaNo ratings yet
- Candesartan RBX PIDocument14 pagesCandesartan RBX PIshadab0123No ratings yet
- Clexane and Clexane Forte : Name of The MedicineDocument20 pagesClexane and Clexane Forte : Name of The MedicineMarin MarianNo ratings yet
- ClexaneDocument19 pagesClexaneahmadNo ratings yet
- FDA NiacinDocument22 pagesFDA NiacinSALSABILA KURNIASIHNo ratings yet
- QuinaprilDocument30 pagesQuinaprilYeyenJaejoongNo ratings yet
- Hypotensive AgentsDocument48 pagesHypotensive AgentsFaizan Ahmad AliNo ratings yet
- Putri RamadhanDocument44 pagesPutri RamadhanRama MulyadiNo ratings yet
- Cardiovascular Agents FarklinDocument66 pagesCardiovascular Agents FarklinBundo NaqueNo ratings yet
- Adalat OrosDocument16 pagesAdalat OrosapniiafniNo ratings yet
- Nitrostat: (Nitroglycerin Sublingual Tablets, USP)Document12 pagesNitrostat: (Nitroglycerin Sublingual Tablets, USP)Ari MartanusaNo ratings yet
- NIFEDIPINE Extended Release Tablets 30 MG, 60 MG, and 90 MGDocument13 pagesNIFEDIPINE Extended Release Tablets 30 MG, 60 MG, and 90 MGXICMENNo ratings yet
- Adalat CC (Nifedipine) Extended Release Tablets: For Oral UseDocument15 pagesAdalat CC (Nifedipine) Extended Release Tablets: For Oral UseRiska AuliahNo ratings yet
- Digitalisanditstoxicity 150130110602 Conversion Gate02Document78 pagesDigitalisanditstoxicity 150130110602 Conversion Gate02Balaji BscRTNo ratings yet
- Azilsartan Medoxomil (Edarbi)Document15 pagesAzilsartan Medoxomil (Edarbi)nicasioaquinoNo ratings yet
- Verapamil PDFDocument13 pagesVerapamil PDFddandan_2No ratings yet
- Dr. Sunatrio - Management Hypovolemic ShockDocument59 pagesDr. Sunatrio - Management Hypovolemic ShockArga Putra SaboeNo ratings yet
- Dosage Adjustment of Cytotoxics in Renal ImpairmentDocument24 pagesDosage Adjustment of Cytotoxics in Renal ImpairmenthamzaNo ratings yet
- S 025 LBLDocument16 pagesS 025 LBLarmanNo ratings yet
- Critical Care CasesDocument7 pagesCritical Care CasesJude Micko Bunyi AlipitNo ratings yet
- TrandolaprilDocument28 pagesTrandolaprilYeyenJaejoongNo ratings yet
- Arixtra: (Fondaparinux Sodium) InjectionDocument26 pagesArixtra: (Fondaparinux Sodium) InjectionTri Purma SariNo ratings yet
- Urea Darah (BUN) 24 MG/DL Kreatinin 1,1 Mg/dl. Pasien Diberi Dosis Loading 0,25 MG / Hari. PadaDocument8 pagesUrea Darah (BUN) 24 MG/DL Kreatinin 1,1 Mg/dl. Pasien Diberi Dosis Loading 0,25 MG / Hari. PadaDwijayanti LestariNo ratings yet
- Jurnal LisinoprilDocument7 pagesJurnal LisinoprildidiisafitriNo ratings yet
- Yang Et Al 2004 Nicardipine Versus Nitroprusside Infusion As Antihypertensive Therapy in Hypertensive EmergenciesDocument6 pagesYang Et Al 2004 Nicardipine Versus Nitroprusside Infusion As Antihypertensive Therapy in Hypertensive EmergenciesButyl KamonphunNo ratings yet
- Dapoxetine Hydrochloride Prescribing InformationDocument17 pagesDapoxetine Hydrochloride Prescribing InformationAdnan TowfiqueNo ratings yet
- Milrinone 1Document8 pagesMilrinone 1Dian Sulistya EkaputriNo ratings yet
- Drug Analysis: AdultsDocument2 pagesDrug Analysis: AdultsFerdinand Sherwin MorataNo ratings yet
- Cardiac ArrhythmiaDocument101 pagesCardiac ArrhythmiaYuvraj ChauhanNo ratings yet
- Cardio Lab MedsDocument11 pagesCardio Lab MedsDianne Erika MeguinesNo ratings yet
- S 084 LBLDocument17 pagesS 084 LBLSusiYanuariNo ratings yet
- Tugas DR Yoma AncaDocument30 pagesTugas DR Yoma Ancaaby mayuNo ratings yet
- Acute Kidney InjuryDocument25 pagesAcute Kidney Injuryradhakishan.22phpp09No ratings yet
- Drugs Acting On The Cardiovascular System-1Document28 pagesDrugs Acting On The Cardiovascular System-1gregorydonald315No ratings yet
- VOLTAREN-diclofenac Sodium D/R Tablet, Delayed Release Direct - RXDocument17 pagesVOLTAREN-diclofenac Sodium D/R Tablet, Delayed Release Direct - RXVân HoàngNo ratings yet
- 2010 Stuard Pycnogenol Improves Kidney Function in Metabolic SyndromeDocument6 pages2010 Stuard Pycnogenol Improves Kidney Function in Metabolic Syndromeindoglo1No ratings yet
- Effect of Losartan Versus Candesartan On Uric Acid, Renal Function, and Fibrinogen in Patients With Hypertension and Hyperuricemia Associated With DiureticsDocument6 pagesEffect of Losartan Versus Candesartan On Uric Acid, Renal Function, and Fibrinogen in Patients With Hypertension and Hyperuricemia Associated With DiureticsNandy Surya KusumaNo ratings yet
- Xylocard PiDocument11 pagesXylocard PiRamakant SharmaNo ratings yet
- Faculty of Physical TherapyDocument15 pagesFaculty of Physical TherapyDr Abdallah BahaaNo ratings yet
- Antidiabetics + ACE Inhibitors: Clinical EvidenceDocument9 pagesAntidiabetics + ACE Inhibitors: Clinical EvidenceGalih SamodraNo ratings yet
- Repaglinide LDocument19 pagesRepaglinide LbigbullsrjNo ratings yet
- IsdnDocument5 pagesIsdnWidya JelitaNo ratings yet
- Integrated Therapeutics II: January 2020Document700 pagesIntegrated Therapeutics II: January 2020Seyoum Tumsa100% (1)
- LanoxinDocument2 pagesLanoxinCris Tan100% (1)
- NeseritideDocument28 pagesNeseritideNavojit Chowdhury100% (1)
- Aki and CKD Therapy 2021Document46 pagesAki and CKD Therapy 2021Alfathri YunediNo ratings yet
- Lanoxin: (Digoxin) InjectionDocument35 pagesLanoxin: (Digoxin) InjectionZainNo ratings yet
- Midterms Topic 3Document19 pagesMidterms Topic 3Lara GatbontonNo ratings yet
- 3 DrugsforHeartFailureDocument60 pages3 DrugsforHeartFailureJov CelNo ratings yet
- Antidysrhythmic Drugs: Dr. SanoozDocument104 pagesAntidysrhythmic Drugs: Dr. SanoozsanoozarmNo ratings yet
- A Pilot Study On The Effect of Telmisartan & Ramipril On 24 H Blood Pressure Profile & Dipping Pattern in Type 1 Diabetes Patients With NephropathyDocument6 pagesA Pilot Study On The Effect of Telmisartan & Ramipril On 24 H Blood Pressure Profile & Dipping Pattern in Type 1 Diabetes Patients With Nephropathydini hanifaNo ratings yet
- Contrast Induced Nephropathy: September 2007Document12 pagesContrast Induced Nephropathy: September 2007usmanmekanNo ratings yet
- Anusha Inotropes 21Document62 pagesAnusha Inotropes 21twister4No ratings yet
- S 038 LBLDocument14 pagesS 038 LBLFarash farshiNo ratings yet
- 017407s034lbl PDFDocument8 pages017407s034lbl PDFNexi anessaNo ratings yet
- Cover Syl TabDocument14 pagesCover Syl TabTEte TEteNo ratings yet
- Digoxi N: Therapeutic Drug Monitoring ofDocument17 pagesDigoxi N: Therapeutic Drug Monitoring ofsky.blueNo ratings yet
- Comprehensive Management of Prostate Cancer 20150821Document30 pagesComprehensive Management of Prostate Cancer 20150821Marhama FitrianiNo ratings yet
- Slide Fraktur FemurDocument26 pagesSlide Fraktur FemurMarhama FitrianiNo ratings yet
- Pitfall in Management of Neonatal Urogenital Disorder 21 08 15Document24 pagesPitfall in Management of Neonatal Urogenital Disorder 21 08 15Marhama FitrianiNo ratings yet
- Controlling Iodine Deficiency Disorder PDFDocument100 pagesControlling Iodine Deficiency Disorder PDFMarhama FitrianiNo ratings yet
- Your Guide To Hearing AidsDocument20 pagesYour Guide To Hearing AidsMarhama FitrianiNo ratings yet
- Hearing Aid BookDocument30 pagesHearing Aid BookwaleedyehiaNo ratings yet
- Controlling Iodine Deficiency DisorderDocument100 pagesControlling Iodine Deficiency DisorderMarhama FitrianiNo ratings yet
- Tugas Biologi Molekuler: Prof. Dr. Muh. Nasrum Massi, PHDDocument1 pageTugas Biologi Molekuler: Prof. Dr. Muh. Nasrum Massi, PHDMarhama FitrianiNo ratings yet
- Simpson's ForensicDocument264 pagesSimpson's ForensicEllagEsz100% (3)
- Prof. Dr. Dr. Rukiah Syawal, SPM (K)Document22 pagesProf. Dr. Dr. Rukiah Syawal, SPM (K)Ronald Ariyanto WiradirnataNo ratings yet
- Glaucoma: Dr. Noro Waspodo, SP.MDocument47 pagesGlaucoma: Dr. Noro Waspodo, SP.MAbd Malik NasNo ratings yet
- How To Prepare Vascular Access 2015Document61 pagesHow To Prepare Vascular Access 2015Marhama FitrianiNo ratings yet
- Influencing Factors For Late-Onset PreclampsiaDocument6 pagesInfluencing Factors For Late-Onset PreclampsiaMarhama FitrianiNo ratings yet
- Prosthesis After Amputation MABIDocument36 pagesProsthesis After Amputation MABIMarhama FitrianiNo ratings yet
- Influencing Factors For Late-Onset PreclampsiaDocument6 pagesInfluencing Factors For Late-Onset PreclampsiaMarhama FitrianiNo ratings yet
- Lion Air - 03 Aug 2014 - YpnoalDocument2 pagesLion Air - 03 Aug 2014 - YpnoalNovita WulandariNo ratings yet
- Bariatric Sleeve GastrectomyDocument34 pagesBariatric Sleeve GastrectomyMarhama FitrianiNo ratings yet
- Hypertension 2008 Valensise 873 80Document9 pagesHypertension 2008 Valensise 873 80Marhama FitrianiNo ratings yet
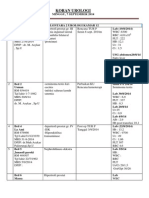
- Koran UrologiDocument28 pagesKoran UrologiMarhama FitrianiNo ratings yet
- Koran Uro Rabu 10 SeptemberDocument2 pagesKoran Uro Rabu 10 SeptemberMarhama FitrianiNo ratings yet
- SIL (2011) List of Semantic DomainsDocument19 pagesSIL (2011) List of Semantic DomainsTakashi NakagawaNo ratings yet
- Principles of Anatomy and Physiology: The Endocrine SystemDocument84 pagesPrinciples of Anatomy and Physiology: The Endocrine SystemTheresia Avila KurniaNo ratings yet
- Healing Psoriasis by Dr. PaganoDocument3 pagesHealing Psoriasis by Dr. PaganoXavier GuarchNo ratings yet
- Pentavet Homeopathic Veterinary Medicine For AnorexiaDocument16 pagesPentavet Homeopathic Veterinary Medicine For AnorexiaLonely WolfNo ratings yet
- Measles Virus (Rubeola) : Anne A. GershonDocument10 pagesMeasles Virus (Rubeola) : Anne A. GershonTammy Utami DewiNo ratings yet
- HIDROKELDocument6 pagesHIDROKELAmara PutraNo ratings yet
- Animal Welfare Act of 1998 As AmendedDocument4 pagesAnimal Welfare Act of 1998 As AmendedRex SagauinitNo ratings yet
- Development of The Nervous SystemDocument5 pagesDevelopment of The Nervous SystemChaGonzalesNo ratings yet
- Acid PhosDocument9 pagesAcid PhosRaveendra MungaraNo ratings yet
- Lec1 WildlifeDocument22 pagesLec1 WildlifeAkhshayaaNo ratings yet
- Pathognomonic Signs of DiseasesDocument4 pagesPathognomonic Signs of DiseasesmydewyboyNo ratings yet
- Subcutaneous MycosesDocument22 pagesSubcutaneous MycosesIan MosesNo ratings yet
- Maternal Stages of Labor and BirthDocument7 pagesMaternal Stages of Labor and BirthFull ErosNo ratings yet
- WDJ 0709Document24 pagesWDJ 0709健康生活園Healthy Life GardenNo ratings yet
- Indian Meat Industry: Opportunities and Challenges: January 2011Document7 pagesIndian Meat Industry: Opportunities and Challenges: January 2011satyajitNo ratings yet
- Biological Science ReviewDocument14 pagesBiological Science ReviewMarjenneilNo ratings yet
- CT Mbbs by DR ShamolDocument197 pagesCT Mbbs by DR ShamolSiva Sandeep Chennimalai50% (2)
- Vegan - The Healthiest DietDocument32 pagesVegan - The Healthiest DietVegan Future100% (4)
- (INFEKSI) - FKUI - Nelwan Score Typhoid Fever.2016Document10 pages(INFEKSI) - FKUI - Nelwan Score Typhoid Fever.2016Yolanda FitrianiNo ratings yet
- Hepatitis B Cases StudiesDocument53 pagesHepatitis B Cases Studiesrieza_huseinNo ratings yet
- MC Question Bank For Quiz 2Document11 pagesMC Question Bank For Quiz 2necrodamien100% (1)
- 2 Medrega Cristian Gabriel enDocument1 page2 Medrega Cristian Gabriel enCristian GabrielNo ratings yet
- Modul Final Biologi Form 4 Fasa 1 2021Document60 pagesModul Final Biologi Form 4 Fasa 1 2021Manmohon Kaur100% (1)
- THE INCONCEIVABLE LIFE OF QUINN Chapter SamplerDocument31 pagesTHE INCONCEIVABLE LIFE OF QUINN Chapter SamplerAbrams BooksNo ratings yet
- Editorial For December 2010 - Rare RemediesDocument4 pagesEditorial For December 2010 - Rare Remediespanniyin selvanNo ratings yet
- 1 Introduction and Ideal OcclusionDocument33 pages1 Introduction and Ideal OcclusionJASPREETKAUR0410100% (1)
- Trial Spm-Bio k2 SkemaDocument14 pagesTrial Spm-Bio k2 SkemaFarah Shafiqah AmiruddinNo ratings yet
- BBLB CB SMK 13-12-18Document16 pagesBBLB CB SMK 13-12-18niaNo ratings yet
- DLLDocument7 pagesDLLmichelle abianNo ratings yet
- Notes 02 Clinical Chemistry 2Document6 pagesNotes 02 Clinical Chemistry 2Brent LagartoNo ratings yet