You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- PROM, UgandanDocument9 pagesPROM, UgandanDavid Eka PrasetyaNo ratings yet
- Obstet Gynecol Clin N Am 33 Myoma UteriDocument37 pagesObstet Gynecol Clin N Am 33 Myoma UteriDavid Eka PrasetyaNo ratings yet
- Ultrasound Study of Ovarian Cysts in Pregnancy Prevalence and SignificanceDocument4 pagesUltrasound Study of Ovarian Cysts in Pregnancy Prevalence and SignificanceDavid Eka PrasetyaNo ratings yet
- Thrombocytopenia in PregnancyDocument18 pagesThrombocytopenia in PregnancyDavid Eka PrasetyaNo ratings yet
- Factors Predictive of Neonatal Thrombocytopenia in Pregnant Women With Immune ThrombocytopeniaDocument7 pagesFactors Predictive of Neonatal Thrombocytopenia in Pregnant Women With Immune ThrombocytopeniaDavid Eka PrasetyaNo ratings yet
- Obstetric Opinions Regarding The Metode of Delivery in Women Had Surgery For Retinal DetachmentDocument4 pagesObstetric Opinions Regarding The Metode of Delivery in Women Had Surgery For Retinal DetachmentDavid Eka PrasetyaNo ratings yet
- Herlina 16.30-20.00Document1 pageHerlina 16.30-20.00David Eka PrasetyaNo ratings yet
- ICD 10 Codes Maternal Care For Cervical Incompetence O34.29 Icd 9 CM Repair Internal Cervical of Cerclage of Ithmus UteriDocument1 pageICD 10 Codes Maternal Care For Cervical Incompetence O34.29 Icd 9 CM Repair Internal Cervical of Cerclage of Ithmus UteriDavid Eka PrasetyaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Business ProposalDocument2 pagesBusiness ProposalKatrina CaveNo ratings yet
- Individual Maternal and Child Health Case Study: Saint Mary's UniversityDocument5 pagesIndividual Maternal and Child Health Case Study: Saint Mary's UniversityCarelle Faith Serrano AsuncionNo ratings yet
- LESSON PLAN On Maternal Mortality and Morbidity FinalDocument17 pagesLESSON PLAN On Maternal Mortality and Morbidity FinalYerra SukumalaNo ratings yet
- Health Educ Handout #11Document3 pagesHealth Educ Handout #11Ram AugustNo ratings yet
- Gender and Food SystemsDocument23 pagesGender and Food SystemsAmbica SumbriaNo ratings yet
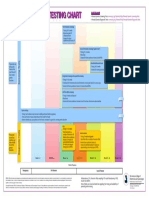
- Prenatal Genetic Testing ChartDocument1 pagePrenatal Genetic Testing ChartMorningDewNo ratings yet
- 94+151A+ ++revisi+ +Zita+Atzmardina Revisi+Edited+FINAL+1527 1534Document8 pages94+151A+ ++revisi+ +Zita+Atzmardina Revisi+Edited+FINAL+1527 1534Iska AlamsyahNo ratings yet
- Bangsal GIN MG 1Document10 pagesBangsal GIN MG 1Iman Ru-ancaNo ratings yet
- Biochemical Methods ObgDocument25 pagesBiochemical Methods ObgRupali AroraNo ratings yet
- Seminar On Various Child Birth Practice, PositionDocument26 pagesSeminar On Various Child Birth Practice, PositionPiyush Dutta100% (1)
- Abdul Halim, Abu Sayeed Md. Abdullah, Fazlur Rahman, Animesh BiswasDocument11 pagesAbdul Halim, Abu Sayeed Md. Abdullah, Fazlur Rahman, Animesh BiswasNoraNo ratings yet
- Episiotomy Case and Postpartum HemorrhageDocument2 pagesEpisiotomy Case and Postpartum HemorrhageRoni NurdiantoNo ratings yet
- Antenatal CareDocument50 pagesAntenatal CareHari HardanaNo ratings yet
- Neonatal Resuscitation: DR Hassan Abdullahi ElechiDocument17 pagesNeonatal Resuscitation: DR Hassan Abdullahi ElechiHadiza Adamu AuduNo ratings yet
- Partogram Professor Adel Abul-Heija FRCOGDocument45 pagesPartogram Professor Adel Abul-Heija FRCOGNizar Rabadi100% (1)
- Group 2: Scenario ADocument47 pagesGroup 2: Scenario Adiza hanniNo ratings yet
- Obs Gyn ClerkingDocument5 pagesObs Gyn ClerkingdonaldooiNo ratings yet
- Differentiation Between True and False Labor ContractionDocument10 pagesDifferentiation Between True and False Labor Contractionpearl joy holleroNo ratings yet
- Sinusoidal and Saltatory Patterns: Unusual Fetal Heart Rate PatternsDocument5 pagesSinusoidal and Saltatory Patterns: Unusual Fetal Heart Rate PatternsMaria MogosNo ratings yet
- Hubungan Usia Dengan EmesisDocument7 pagesHubungan Usia Dengan EmesisNahar RuddinNo ratings yet
- Antenatal Care For Uncomplicated PregnanciesDocument69 pagesAntenatal Care For Uncomplicated PregnanciesJony SaputraNo ratings yet
- Premature Rupture of MembranesDocument3 pagesPremature Rupture of MembranesSheena Kunkel100% (2)
- Antepartum HaemorrhageDocument36 pagesAntepartum HaemorrhageAfi RamadaniNo ratings yet
- CDEM 17jan Complete WEBDocument24 pagesCDEM 17jan Complete WEBRicardo Jonathan Ayala GarciaNo ratings yet
- SOAL ObsgynDocument24 pagesSOAL ObsgynmadeprasetyawardanaNo ratings yet
- Pregnant Dog - Pregnancy Signs in Dogs - Dog Article On Pets - Ca What To Expect When Your Dog Is ExpectingDocument3 pagesPregnant Dog - Pregnancy Signs in Dogs - Dog Article On Pets - Ca What To Expect When Your Dog Is Expectingmale nurseNo ratings yet
- Cesarean Delivery and Peripartum HysterectomyDocument26 pagesCesarean Delivery and Peripartum HysterectomyPavan chowdaryNo ratings yet
- Answer Key Midwifery 1 Final Term ExaminationDocument6 pagesAnswer Key Midwifery 1 Final Term Examinationgladz25No ratings yet
- Social and Preventive PediatricsDocument11 pagesSocial and Preventive PediatricssreekalaNo ratings yet
- 3 - Intrapartum CareDocument97 pages3 - Intrapartum CareRem AlfelorNo ratings yet