You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
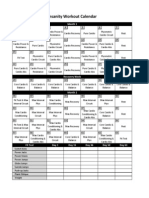
- Cronograma InsanityDocument1 pageCronograma InsanityCatherine EcheverryNo ratings yet
- Analysis of The Pattern of Suprahyoid Muscle Activity During Pharyngeal Swallowing of Foods by Healthy Young SubjectsDocument7 pagesAnalysis of The Pattern of Suprahyoid Muscle Activity During Pharyngeal Swallowing of Foods by Healthy Young SubjectsFabian Esteban SubiabreNo ratings yet
- Roberto Merletti, Multi Channel Surface EMG For The Non Invasive Assessment of The Anal Sphincter Muscle 2004 Digestion PortoDocument26 pagesRoberto Merletti, Multi Channel Surface EMG For The Non Invasive Assessment of The Anal Sphincter Muscle 2004 Digestion PortoFabian Esteban SubiabreNo ratings yet
- Analysis of The Pattern of Suprahyoid Muscle Activity During Pharyngeal Swallowing of Foods by Healthy Young SubjectsDocument7 pagesAnalysis of The Pattern of Suprahyoid Muscle Activity During Pharyngeal Swallowing of Foods by Healthy Young SubjectsFabian Esteban SubiabreNo ratings yet
- Antagonistas de Los Receptores NMDA Dolor CrónicoDocument13 pagesAntagonistas de Los Receptores NMDA Dolor CrónicoMario Viazcan CarbajalNo ratings yet
- 1984 Early Physiotherapy in The Treatment of Spastic DiplegiaDocument7 pages1984 Early Physiotherapy in The Treatment of Spastic DiplegiaFabian Esteban SubiabreNo ratings yet
- Deluca Surface Electromyography Detection&RecordingDocument10 pagesDeluca Surface Electromyography Detection&RecordingJuan Rodriguez IIINo ratings yet
- Early Intervention in The NeurodevelopmentDocument6 pagesEarly Intervention in The NeurodevelopmentFabian Esteban Subiabre100% (1)
- Depuracion de Mucus en Las Vias AereasDocument7 pagesDepuracion de Mucus en Las Vias AereasFabian Esteban SubiabreNo ratings yet
- NAVA HypoventilationDocument3 pagesNAVA HypoventilationFabian Esteban SubiabreNo ratings yet
- Ooool - Biomecanica Craneo - Cervical y ATMDocument30 pagesOoool - Biomecanica Craneo - Cervical y ATMFabian Esteban SubiabreNo ratings yet
- Prevention of Endotracheal Suctioning-Induced Alveolar Derecruitment in Acute Lung InjuryDocument54 pagesPrevention of Endotracheal Suctioning-Induced Alveolar Derecruitment in Acute Lung InjuryFabian Esteban SubiabreNo ratings yet
- Update en EpocDocument9 pagesUpdate en EpocFabian Esteban SubiabreNo ratings yet
- Ventlacionmecanica ASMADocument10 pagesVentlacionmecanica ASMAFabian Esteban SubiabreNo ratings yet
- 2015 Early Mobilization in The Critical Care Unit, A Review of Adult and Pediatric LiteratureDocument9 pages2015 Early Mobilization in The Critical Care Unit, A Review of Adult and Pediatric LiteratureFabian Esteban SubiabreNo ratings yet
- Physiology of Mechanical VentilationDocument18 pagesPhysiology of Mechanical VentilationLiliana Andrea Hurtado MeraNo ratings yet
- A Chart of Failure Risk For NoninvasiveDocument8 pagesA Chart of Failure Risk For NoninvasiveFabian Esteban SubiabreNo ratings yet
- Extubation Failure Magnitude of The ProblemDocument8 pagesExtubation Failure Magnitude of The ProblemFabian Esteban SubiabreNo ratings yet
- 116 093 Agustiag Oxygen Therapy During Exacerbations CopdDocument6 pages116 093 Agustiag Oxygen Therapy During Exacerbations CopdFabian Esteban SubiabreNo ratings yet
- The Effects of Orthostatism in Adult Intensive Care Unit PatientsDocument8 pagesThe Effects of Orthostatism in Adult Intensive Care Unit PatientsFabian Esteban SubiabreNo ratings yet
- Endotracheal Suctioning of Mechanically Ventilated Patients With Artificial Airways (June 2010)Document7 pagesEndotracheal Suctioning of Mechanically Ventilated Patients With Artificial Airways (June 2010)DCaeiroNo ratings yet
- Citacion Vancouver PapersDocument1 pageCitacion Vancouver PapersFabian Esteban SubiabreNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Blood Gas AnalyzerDocument36 pagesBlood Gas AnalyzerNabila Souza NugrahaNo ratings yet
- Blood GasDocument31 pagesBlood GasHusna Nur FitrianaNo ratings yet
- The Instillment of Saline in Suctioning EbpDocument46 pagesThe Instillment of Saline in Suctioning Ebpapi-340261639100% (6)
- Miller 7th Ed Chapter I HistoryDocument35 pagesMiller 7th Ed Chapter I Historyjbahalkeh7570No ratings yet
- ABG WorksheetDocument10 pagesABG WorksheetRacquel PinnockNo ratings yet
- Medical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 68Document10 pagesMedical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 68sarasjunkNo ratings yet
- Electrolytes Used in Acid-Base TheraphyDocument30 pagesElectrolytes Used in Acid-Base TheraphySuresh ThanneruNo ratings yet
- Pulmonary Pathophysiology The Essentials-2013-CDDocument196 pagesPulmonary Pathophysiology The Essentials-2013-CDMaria Spatari100% (2)
- Aspiration PneumoniaDocument16 pagesAspiration PneumoniaFeni DianiNo ratings yet
- Respiratory Failure MCQ and QuestionsDocument5 pagesRespiratory Failure MCQ and QuestionsChikezie Onwukwe67% (3)
- Nclex 2Document147 pagesNclex 2Habet Fidem100% (5)
- Formative 1 - Ans KeyDocument47 pagesFormative 1 - Ans KeyDhine Dhine ArguellesNo ratings yet
- Adjusting Ventilator SettingsDocument7 pagesAdjusting Ventilator SettingsSiva RamanNo ratings yet
- Heart Failure Care Plan LippincottDocument62 pagesHeart Failure Care Plan LippincottDyllano100% (1)
- CP Acute Renal Failure Chap7Document128 pagesCP Acute Renal Failure Chap7Katherine 'Chingboo' Leonico LaudNo ratings yet
- American Thoracic Society - Interpretation of Arterial Blood Gases (ABGs)Document7 pagesAmerican Thoracic Society - Interpretation of Arterial Blood Gases (ABGs)humberto_2No ratings yet
- QADocument11 pagesQAGladys FernandezNo ratings yet
- Mechanical VentilationDocument43 pagesMechanical VentilationsalemraghuNo ratings yet
- Abg CaseAnswersDocument7 pagesAbg CaseAnswersDiana HyltonNo ratings yet
- Arterial Blood Gas Analysis and InterpretationDocument23 pagesArterial Blood Gas Analysis and InterpretationKrutthivaasa PriyaNo ratings yet
- Respiratory SystemDocument356 pagesRespiratory Systembaba saiprem83% (6)
- Arterial Blood Gas Cases: Case 1Document4 pagesArterial Blood Gas Cases: Case 1Diana HyltonNo ratings yet
- CCRN Sample QuestionsDocument5 pagesCCRN Sample Questionsgwapdose50% (2)
- Exercises in Acid and Base Disorders 2Document3 pagesExercises in Acid and Base Disorders 2Marisa MonplaisirNo ratings yet
- Arterial Blood GasesDocument44 pagesArterial Blood GasesRidhwan Mgt100% (1)
- Arterial Blood GasDocument6 pagesArterial Blood GasnsfanfoinNo ratings yet
- AbgDocument8 pagesAbgprecillathoppilNo ratings yet
- Acido Base NEJMDocument12 pagesAcido Base NEJMUlises de ÍtacaNo ratings yet
- (Osborn) Chapter 19: Learning Outcomes (Number and Title)Document28 pages(Osborn) Chapter 19: Learning Outcomes (Number and Title)Kitties100% (1)
- Basic Chest X-Ray InterpretationDocument40 pagesBasic Chest X-Ray InterpretationEzekiel Arteta0% (1)