RISK &
CAUSATION
FRANCES AVILES
MD MPH BSC
�COHORT STUDY
Cohort: group of people who share a common
characteristic
Identifies people with risk factors and
compares disease incidence to incidence rate in
another group of people without those risk
factors.
Connects Incidence to a Causality
Large Sample Sizes
Expensive/Time Consuming
�COHORT STUDY: RISK FACTOR
EXPOSURE
PROSPECTIVE: Towards the future; follows disease
incidence (MC)
RETROSPECTIVE: Looks into past archived data
Prospective studies follow a cohort into the future
for a health outcome.
Retrospective studies trace the cohort back in
time for exposure information after the outcome
has occurred. Retrospective studies group
subjects based on their exposure status and
compare their incidence of disease.
�Prospective Cohort
In a Hospital A group of heavy smokers and a
group of non-smokers are selected for a cohort
study. Lung Cancer incidence is assessed for the
following 5 years.
�Retrospective Cohort
�Start
?
Exposur
e
Time
Disease
�Cohort Study
outcome is measured after exposure
yields true incidence rates and relative risks
may uncover unanticipated associations with outcome
best for common outcomes
expensive
requires large numbers
takes a long time to complete
prone to attrition bias (compensate by using persontime methods)
prone to the bias of change in methods over time
�CASE CONTROL STUDY:
DISEASE
Uses a group of people with disease and a
matching group of non-diseased people
(CONTROL)
RETROSPECTIVE: Looks back in time for the
presence or absence of risk factors.
Looks for causality of risk factors by analyzing
the presence of risk factors in patients with given
disease and the absence of these RFs in the
selected patients that are not diseased.
�CASE CONTROL
In a hospital- A group of pts with LUNG CANCER is
selected along with a group without LUNG
CANCER. Smoking habits are assessed for each
group.
�Start
?
Disease
LOOK
BACK
Exposur
e
�Case Control
outcome is measured before exposure
controls are selected on the basis of not having
the outcome
good for rare outcomes
relatively inexpensive
smaller numbers required
quicker to complete
prone to selection bias
prone to recall/retrospective bias
�Risk
& Measurements
of Risk and Effect
�RISK
To analyze a Study, Risk needs to be assessed
Risk: the proportion of persons who are unaffected
at the beginning of a study period, but who could
possibly experience an event (e.g., death, disease,
or injury) during the study period
Quantifying Risk: Relative risk, attributable risk,
and the odds (or odds risk) ratio are measures
used to quantify risk in population studies
�The knowledge that something is a risk factor
for a disease can be used to help:
Prevent the disease.
Predict its future incidence and prevalence.
Diagnose it (diagnostic suspicions are higher if it is
known that a patient was exposed to the risk factor).
Establish the cause of a disease of unknown
etiology.
�Absolute Risk
The fundamental measure of risk is
incidence. The incidence of a disease is, in
fact, the absolute risk of contracting it.
If the INCIDENCE of disease is 10 per 10,000 people per Yr.
Then the ABSOLUTE RISK of a person actually contracting it
is also 10 per 1,000 per Yr., or 1% per Yr.
�Measures of RISK & EFFECT
Measures of effect to being exposed to a risk factor on the
risk of contracting a disease.
A number of different comparisons of risk can be made,
including relative risk, attributable risk, and the odds
ratio.
�Relative risk (RR)
How
many times exposure to the risk
factor increases the risk of contracting
the disease.
It is therefore the ratio of the incidence of the disease among
exposed persons to the incidence of the disease among
unexposed person
Because relative risk is a ratio of risks, it is sometimes called
the risk ratio, or morbidity ratio. In the case of outcomes
involving death, rather than just disease, it may also be called
the mortality ratio.
�Relative Risk (RR)
RELATIVE RISK : is the group more or less likely to develop
DZ?
[RR= INCIDENCE IN EXPOSED/INCIDENCE IN
UNEXPOSED]
For example, the incidence rate of lung cancer among smokers in
New Jersey is 20/1000, while the incidence rate of lung cancer
among nonsmokers in New Jersey is 2/1000.
Therefore, the chance of getting lung cancer (the relative risk) for this
New Jersey population is ?
�RELATIVE RISK REDUCTION
The proportion of risk reduction attributable to the intervention as
compared to a control.
RRR= 1 - relative risk
RRR= AR/IH
IH= highest incident rate
IL= lowest incident rate
Reports of risk reductions due to treatments in many clinical trials, and in
almost all pharmaceutical advertisements, are of relative risk reductions
There were 73 deaths from cardiovascular causes in the placebo
group (3293 men); the cardiovascular mortality rate was
therefore 73/3,293 = 0.022 (2.2%) in this group.
In the pravastatin group (3,302 men), there were 50
cardiovascular deaths, giving a mortality rate of 50/3,302 =
0.015, or 1.5%.
The RR of death in those given the drug is 1.5/2.2 = 0.68,
The RRR is (1 - 0.68)=0.32, or 32% showing that an impressive
32% of cardiovascular deaths were prevented by the drug.
The ARR is (2.2% - 1.5%) = 0.7% a far less impressivesounding figure, showing that of all men given the drug for 4.9
years, 0.7% of them were saved from a cardiovascular death.
�ATTRIBUTABLE RISK (AR)
The additional incidence of a disease that is attributable to the risk
factor in question. The difference in risk between exposed and
unexposed groups, or the proportion of disease occurrences that are
attributable to the Exposure
ATTRIBUTABLE RISK: how many more cases?
[AR= INCIDENCE RATE IN EXPOSED-INCIDENCE RATE IN UNEXPOSED]
Then, the risk of lung cancer attributable to smoking (the attributable risk) in this New
Jersey population is 20/1000 minus 2/1000 or 18/1000.
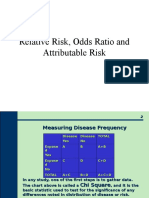
�2X2 Table
RISK EXPOSURE
UNEXPOSED
DZ
NO DZ
TOTAL
a+b
c+d
How many were exposed
How many were not exposed
How many How many do not
have disease
have disease
*Incidence in Exposed: a/a+b
*Incidence in Unexposed: c/c+d
Attributable Risk and Relative Risk are mainly
used for Cohorts Studies
Odds Ratio are commonly used for Case Control
Studies
�Attributable Risk Reduction
The difference in risk attributable to the
intervention as compared to control
Risk of intervention group Risk of Control Group
�Absolute Difference of Risk
Risk difference is the risk in the exposed group
minus the risk in the unexposed group.
If an exposure is harmful (as in the case of
cigarette smoking), the risk difference is
expected to be greater than 0.
If an exposure is protective (as in the case of a
vaccine), the risk difference is expected to be
less than 0.
Risk difference is also known as attributable risk.
Rate difference (absolute difference in rate) is
the rate in the exposed group minus the rate in
�ATTRIBUTABLE RISK PERCENT
Percent of cases due to exposure
Used to assess proportion of cases
due to risk factor.
AR%= RR-1/RR
�NUMBER NEEDED TO TREAT: NNT
NUMBER NEEDED TO HARM: NNH
PREVENTION: NNT
CAUSALITY: NNH
How many have to do something to prevent one
case of disease
How many would have to stop smoking? - NNT
How many pts would have to smoke? - NNH
�Number needed to Treat
Number of patients who need to be treated for 1
patient to benefit.
NNT=1/ARR.
�Number needed to Harm
Number of patients who need to be exposed to a
risk factor for 1 patient to be harmed.
NNH=1/AR
�ODDS RATIO
ODDS RATIO: Estimates the increased odds of having
risk factors when comparing disease and non-diseased
groups
[OR=ad/bc]
Not a prediction of disease
Estimates the
strength of risk factors.
Since incidence data are not available in a case-control study, the odds ratio can be
used as an estimate of relative risk when a disease is uncommon
� Of 200 patients in the hospital, 50 have lung cancer. Of
these 50 patients, 45 are smokers.
Of the remaining 150 hospitalized patients who do not
have lung cancer, 60 are smokers.
Use this information to calculate the odds ratio for
smoking and the risk of lung cancer.
People with lung cancer A = 45 B = 5
People without lung cancer C = 60 D = 90
(A)(D) (45)(90) / (B)(C) (5)(60)
4050/300= OR=13.5
An odds ratio of 13.5 means that the risk of lung cancer is
13.5 times higher in peoplewho smoke than in those who
do not smoke.
�CAUSATION
�CONCEPT OF CAUSE
An understanding of the causes of disease is
important in the health field not only for
prevention but also in diagnosis and the
application of treatment.
A cause of a disease is an event, condition,
characteristic, or combination of these factors
which plays an important role in producing the
disease.
A cause could be sufficient or necessary
�SUFFICIENT CAUSE
A cause is termed sufficient when it
inevitably/certainly produces or initiates a disease.
It is not usually a single factor, but often comprises
several components. e.g. cigarette smoking is one
component of the sufficient cause in lung cancer.
In general, it is not necessary to identify all the
components of a sufficient cause before effective
prevention can take place, since the removal of
one component may interfere with the action of
the others and thus prevent the disease.
�NECESSARY CAUSE
A cause is termed necessary if a disease
cannot develop in its absence.
Each sufficient cause has a necessary cause
as a component.
�Types of Causes
Sufficient - If the cause is present, disease will
always occur.
Necessary - The cause must be present for the
disease/condition to occur, although it does not
always result in disease (not necessarily
sufficient)
Risk factor - Increases the probability of a
particular disease/condition in a group of people
compared with an otherwise similar group of
people who lack this factor (neither necessary
nor sufficient)
�Variable Associations
�Variable Associations (Example)
�Bidirectional Causality
�Bidirectional
Causality
�Rate and Risk
A rate is a good approximation of risk if the:
Event in the numerator occurs only once
per individual during the study interval
Proportion of the population affected by the
event is small (e.g., less than 5%)
Time interval is relatively short
If the event in the numerator occurs more
than once during the study (e.g., colds, ear
infections, asthma attacks) a related statistic
called incidence density should be used
instead of rate
�Steps in Determining Cause
and Effect
1.Investigation of the statistical association
(Mills Canons)
1.Strength of association
2.Consistency
3.Specificity
4.Biological plausibility
5.Dose response
2.Investigation of the temporal relationship
. Latent periods make onset of risk factors
unclear
3.Elimination of alternative explanations
. Never eliminated fully or indefinitely;
challenged by each new explanation that fits
the data
�Only 4 Possibilities for Any
Association
1.Causal (true association)
2.Chance (based on probability)
3.Random error (non-differential error)
4.Systematic error (bias)
Confounding (special case of bias)
�Specific Types of Rates
�Specific Types of Rates
�Specific Types of Rates
�REFERENCES
1) Katz D, et al. Jekels Epidemiology, Biostatistics, Preventive Medicine,
and Public Health. 4th Ed. Saunders: Philadelphia, PA. 2014.
2) Daugherty S, et al. USMLE, Step 1, Behavioral Science, Epidemiology, &
Biostatistics. Becker Professional Education. 2013.
3) Brown T, Shah S. Biostatistics. USMLE STEP 1 SECRETS. 3rd Ed.
Saunders: Philadelphia, PA. 2013.
4) Principles of Epidemiology in Public Health Practice: An Introduction to
Applied Epidemiology and Biostatistics. Centers for Disease Control and
Prevention. Third Edition. Published 2006. Updated 2011. http://
www.cdc.gov/ophss/csels/dsepd/ss1978/index.html
5) Le T, et al. First Aid for the USMLE Step 1, a Student to Student
Guide. McGraw Hill Education. 2014.
6) Glaser A. High Yield Biostatistics, Epidemiology, and Public Health.
Lippincott Williams and Wilkins; 4th Ed. 2014. Ch 8.