You might also like
- Enhancing Informed Consent For Research and TreatmentDocument13 pagesEnhancing Informed Consent For Research and TreatmentBurnley JenifferNo ratings yet
- Aging and Decision Making: Empirical and Applied PerspectivesFrom EverandAging and Decision Making: Empirical and Applied PerspectivesThomas M. HessNo ratings yet
- Garb - The Representativeness and Past-Behavior Hueristics in Clinical JudgementDocument6 pagesGarb - The Representativeness and Past-Behavior Hueristics in Clinical JudgementNicolas Di PersiaNo ratings yet
- Informed Consent to Psychoanalysis: The Law, the Theory, and the DataFrom EverandInformed Consent to Psychoanalysis: The Law, the Theory, and the DataNo ratings yet
- Inpatient Geriatric Psychiatry: Optimum Care, Emerging Limitations, and Realistic GoalsFrom EverandInpatient Geriatric Psychiatry: Optimum Care, Emerging Limitations, and Realistic GoalsHoward H. FennNo ratings yet
- Dimensional PsychopathologyFrom EverandDimensional PsychopathologyMassimo BiondiNo ratings yet
- C9a1 PDFDocument12 pagesC9a1 PDFfujfrNo ratings yet
- CAMDEX. A Standardised Instrument For The Diagnosis of MentalDocument13 pagesCAMDEX. A Standardised Instrument For The Diagnosis of MentalLeila CamilaNo ratings yet
- Clinical Versus Actuarial Judgment: Methods of Judgment and Means of ComparisonDocument19 pagesClinical Versus Actuarial Judgment: Methods of Judgment and Means of ComparisonanguschandlerNo ratings yet
- Risk Assessment: Origins, Evolution, and Implications for PracticeFrom EverandRisk Assessment: Origins, Evolution, and Implications for PracticeNo ratings yet
- 9/geriatric Depression Scale (GDS) : Clinical GerontologistDocument10 pages9/geriatric Depression Scale (GDS) : Clinical GerontologistTeresa GasparNo ratings yet
- Diagnosis and Treatment of Mental Disorders: An IntroductionFrom EverandDiagnosis and Treatment of Mental Disorders: An IntroductionNo ratings yet
- Availability HeuristicDocument10 pagesAvailability Heuristicapi-440355514No ratings yet
- Detection of Malingering during Head Injury LitigationFrom EverandDetection of Malingering during Head Injury LitigationArthur MacNeill Horton, Jr.No ratings yet
- Neurocognitive Assessments Transgender Adults - LTDocument14 pagesNeurocognitive Assessments Transgender Adults - LTDrNihilismNo ratings yet
- The Identification of Autistic Adults’ Perception of Their Own Diagnostic Pathway: A Research Dissertation Submitted for the Degree of Master of Autism at Sheffield Hallam UniversityFrom EverandThe Identification of Autistic Adults’ Perception of Their Own Diagnostic Pathway: A Research Dissertation Submitted for the Degree of Master of Autism at Sheffield Hallam UniversityNo ratings yet
- Clinical Approach in Autism: Management and Treatment: March 2013Document25 pagesClinical Approach in Autism: Management and Treatment: March 2013Carlos PonceNo ratings yet
- Change or Die: The Three Keys to Change at Work and in LifeFrom EverandChange or Die: The Three Keys to Change at Work and in LifeRating: 3.5 out of 5 stars3.5/5 (30)
- Our Genes, Our Choices: How Genotype and Gene Interactions Affect BehaviorFrom EverandOur Genes, Our Choices: How Genotype and Gene Interactions Affect BehaviorNo ratings yet
- Marsh 2017Document10 pagesMarsh 2017CoordinacionPsicologiaVizcayaGuaymasNo ratings yet
- The Role of The Individual in The Coming Era of Process-Based Therapy (Articulo Examen Final)Document14 pagesThe Role of The Individual in The Coming Era of Process-Based Therapy (Articulo Examen Final)Cristian Steven Cabezas JoyaNo ratings yet
- APA Resource DocumentDocument17 pagesAPA Resource DocumentAxel Robinson HerreraNo ratings yet
- Article MSQOL-54Document21 pagesArticle MSQOL-54bogdanneamtuNo ratings yet
- 10 1016@j Scog 2019 01 001Document7 pages10 1016@j Scog 2019 01 001yohana ncNo ratings yet
- Behavioral Forensics: Using Applied Behavior Analysis in Psychological Court EvaluationsFrom EverandBehavioral Forensics: Using Applied Behavior Analysis in Psychological Court EvaluationsRating: 4 out of 5 stars4/5 (1)
- Restraints in Dementia Care: A Nurse’s Guide to Minimizing Their UseFrom EverandRestraints in Dementia Care: A Nurse’s Guide to Minimizing Their UseNo ratings yet
- Performing Bimanual Activities: The Experiences of Young Persons With Hemiplegic Cerebral PalsyDocument10 pagesPerforming Bimanual Activities: The Experiences of Young Persons With Hemiplegic Cerebral PalsyArriane AlochaNo ratings yet
- Neuroscience D MDocument12 pagesNeuroscience D MEgla AlishollariNo ratings yet
- A Study Guide for Psychologists and Their Theories for Students: CARL ROGERSFrom EverandA Study Guide for Psychologists and Their Theories for Students: CARL ROGERSRating: 4 out of 5 stars4/5 (1)
- A New Clinical Scale For The Staging of DementiaDocument8 pagesA New Clinical Scale For The Staging of Dementiazitamugen.workNo ratings yet
- 8 Substance and Behavioral Addictions Assessment InstrumentsDocument19 pages8 Substance and Behavioral Addictions Assessment InstrumentszuveriaNo ratings yet
- The Essential Family Guide to Borderline Personality Disorder: New Tools and Techniques to Stop Walking on EggshellsFrom EverandThe Essential Family Guide to Borderline Personality Disorder: New Tools and Techniques to Stop Walking on EggshellsRating: 4 out of 5 stars4/5 (9)
- Accuracy of SurrogatesDocument9 pagesAccuracy of SurrogatesScott KimNo ratings yet
- Palliative EBMDocument2 pagesPalliative EBMMichael Spike LevinNo ratings yet
- Example of An Experiment (Self)Document8 pagesExample of An Experiment (Self)Jacqui PendergastNo ratings yet
- The Use of The Johnson Behavioral System Model To Measure Changes During Adolescent Hospitalization PDFDocument13 pagesThe Use of The Johnson Behavioral System Model To Measure Changes During Adolescent Hospitalization PDFGerlyn Lariosa Pag-ongNo ratings yet
- A Literature Review of Findings in Physical Elder AbuseDocument8 pagesA Literature Review of Findings in Physical Elder AbuseafmzxpqoizljqoNo ratings yet
- A2 Psychology Unit 4, ClinicalDocument11 pagesA2 Psychology Unit 4, ClinicalLesley Connor100% (1)
- Not All Patiens Want To ParticipateDocument5 pagesNot All Patiens Want To ParticipateAmelia ArnisNo ratings yet
- The Hindsight Bias A Meta AnalysisDocument22 pagesThe Hindsight Bias A Meta AnalysisGreta Manrique GandolfoNo ratings yet
- Decision-Making Style, Driving Style, and Self-Reported Involvement in Road Traffic AccidentsDocument18 pagesDecision-Making Style, Driving Style, and Self-Reported Involvement in Road Traffic AccidentsOlivia-Rahela PașniciucNo ratings yet
- Hierarchical Taxonomy of Psychopathology (HiTOP) - Kotov, 2018Document2 pagesHierarchical Taxonomy of Psychopathology (HiTOP) - Kotov, 2018Hugo UrquinaNo ratings yet
- Patient Advocacy and DSM-5: Commentary Open AccessDocument5 pagesPatient Advocacy and DSM-5: Commentary Open AccessAKNTAI002No ratings yet
- The Social Rejection of Former Mental Patients: Understanding Why Labels Matter'Document30 pagesThe Social Rejection of Former Mental Patients: Understanding Why Labels Matter'Mikoto NakataNo ratings yet
- Mentally Disordered OffendersDocument14 pagesMentally Disordered OffendersMunteanu SilviaNo ratings yet
- The Treatment of Schizoid Personality Disorder Using Psychodynamic MethodsDocument25 pagesThe Treatment of Schizoid Personality Disorder Using Psychodynamic MethodsnikhilNo ratings yet
- Healing Stem Cells Healing You: Choosing Regenerative Medical Injection Therapy to treat osteoarthritis, tendon tears, meniscal tears, hip and knee injuriesFrom EverandHealing Stem Cells Healing You: Choosing Regenerative Medical Injection Therapy to treat osteoarthritis, tendon tears, meniscal tears, hip and knee injuriesNo ratings yet
- The Massachusetts General Hospital Guide to Depression: New Treatment Insights and OptionsFrom EverandThe Massachusetts General Hospital Guide to Depression: New Treatment Insights and OptionsBenjamin G. ShaperoNo ratings yet
- Wakefield, 1992Document16 pagesWakefield, 1992Luis Fernando Cuji LlugnaNo ratings yet
- Gloria R. Burthold - Psychology of Decision Making in Legal, Health Care and Science Settings-Nova Science Publishers (2007)Document281 pagesGloria R. Burthold - Psychology of Decision Making in Legal, Health Care and Science Settings-Nova Science Publishers (2007)rpc0601No ratings yet
- Stigmatisation of People With Mental Illnesses Stigmatisation of People With Mental IllnessesDocument5 pagesStigmatisation of People With Mental Illnesses Stigmatisation of People With Mental Illnessessri endriyaniNo ratings yet
- The Forensic Examination: A Handbook for the Mental Health ProfessionalFrom EverandThe Forensic Examination: A Handbook for the Mental Health ProfessionalNo ratings yet
- Pharma Compliance Auditing Best PracticesDocument35 pagesPharma Compliance Auditing Best PracticesShah Maqsumul Masrur TanviNo ratings yet
- Assement AuditDocument35 pagesAssement AuditPeter GeorgeNo ratings yet
- Five Ws Internal Audit36700Document13 pagesFive Ws Internal Audit36700Shah Maqsumul Masrur TanviNo ratings yet
- Five Ws Internal Audit36700Document13 pagesFive Ws Internal Audit36700Shah Maqsumul Masrur TanviNo ratings yet
- Internal AuditDocument43 pagesInternal AuditNicoleta ConstantinescuNo ratings yet
- INST 275 Lecture14Document51 pagesINST 275 Lecture14bayern munchenNo ratings yet
- Project Scheduling with OpenProjDocument16 pagesProject Scheduling with OpenProjShah Maqsumul Masrur TanviNo ratings yet
- Role of Internal Audit DepartmentDocument19 pagesRole of Internal Audit DepartmentGuadalupe PenningtonNo ratings yet
- Chapt 1Document22 pagesChapt 1Sidra SwatiNo ratings yet
- Project Scheduling with OpenProjDocument16 pagesProject Scheduling with OpenProjShah Maqsumul Masrur TanviNo ratings yet
- Audit Checklist: RequirementDocument4 pagesAudit Checklist: RequirementShah Maqsumul Masrur TanviNo ratings yet
- INST 275 Lecture14Document51 pagesINST 275 Lecture14bayern munchenNo ratings yet
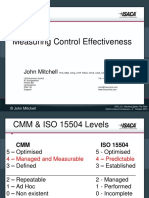
- Measuring Control Effectiveness - John MitchellDocument19 pagesMeasuring Control Effectiveness - John MitchellShah Maqsumul Masrur TanviNo ratings yet
- A Model For Assessing COBIT 5 and ISO 27001 Simultaneously: July 2018Document11 pagesA Model For Assessing COBIT 5 and ISO 27001 Simultaneously: July 2018Shah Maqsumul Masrur TanviNo ratings yet
- Pharma Compliance Auditing Best PracticesDocument35 pagesPharma Compliance Auditing Best PracticesShah Maqsumul Masrur TanviNo ratings yet
- Car Loan Application FormDocument56 pagesCar Loan Application FormShah Maqsumul Masrur TanviNo ratings yet
- Iso 27001Document84 pagesIso 27001sboukhal100% (2)
- CFSA Study GuideDocument312 pagesCFSA Study Guidehossainmz88% (8)
- MD - Mushfiqur RahmanCISA, CLPTP, CCISOProfileDocument10 pagesMD - Mushfiqur RahmanCISA, CLPTP, CCISOProfileShah Maqsumul Masrur TanviNo ratings yet
- Coreworx Interface Management Implementation Webinar October2013Document21 pagesCoreworx Interface Management Implementation Webinar October2013Shah Maqsumul Masrur TanviNo ratings yet
- CRACK TOUGH CISSP EXAMDocument6 pagesCRACK TOUGH CISSP EXAMrahuls256No ratings yet
- Accenture Management Consulting: Advancing The Science of High PerformanceDocument24 pagesAccenture Management Consulting: Advancing The Science of High PerformanceShah Maqsumul Masrur TanviNo ratings yet
- Flourish Your Career With ACME: Executive/ Senior Executive - Corporate LegalDocument1 pageFlourish Your Career With ACME: Executive/ Senior Executive - Corporate LegalShah Maqsumul Masrur TanviNo ratings yet
- Function HierarchyDocument22 pagesFunction HierarchyShah Maqsumul Masrur TanviNo ratings yet
- CH 11Document21 pagesCH 11Shah Maqsumul Masrur TanviNo ratings yet
- ISO27001 - 2013 Implementation RoadmapDocument1 pageISO27001 - 2013 Implementation RoadmapShah Maqsumul Masrur TanviNo ratings yet
- Coreworx Interface Management Basics Webinar October2013Document21 pagesCoreworx Interface Management Basics Webinar October2013Shah Maqsumul Masrur TanviNo ratings yet
- 3 Big Problems For Social Network Analysis FinalDocument2 pages3 Big Problems For Social Network Analysis FinalShah Maqsumul Masrur TanviNo ratings yet
- Accounting MathDocument1 pageAccounting MathShah Maqsumul Masrur TanviNo ratings yet
- Unit 03Document37 pagesUnit 03Shah Maqsumul Masrur TanviNo ratings yet