You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5811)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Chapter 38: Cardiovascular Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument7 pagesChapter 38: Cardiovascular Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Valvular Heart DiseaseDocument43 pagesValvular Heart Diseaseurmila prajapatiNo ratings yet
- Dr. Anas Yasin - MDDocument58 pagesDr. Anas Yasin - MDMahfouzNo ratings yet
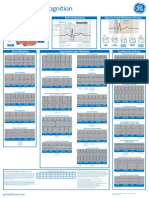
- Arrhythmia Recognition Part 1 and 2 DOC1178264 Rev2Document2 pagesArrhythmia Recognition Part 1 and 2 DOC1178264 Rev2Nico Angelo CopoNo ratings yet
- Almaghrabi Cardio ExaminationDocument22 pagesAlmaghrabi Cardio ExaminationSagit Nauman81No ratings yet
- Cardiology MnemonicsDocument12 pagesCardiology MnemonicsEliza SparkNo ratings yet
- Congenital Heart Disease - ASDDocument36 pagesCongenital Heart Disease - ASDAuni Akif Aleesa100% (1)
- Daftar Tarif Ina CBG'S: NIRA 32740043589 NO Diagnosa KodeDocument8 pagesDaftar Tarif Ina CBG'S: NIRA 32740043589 NO Diagnosa KodeAgus NugrahaNo ratings yet
- Grade 1 Pattern of LV Diastolic FillingDocument3 pagesGrade 1 Pattern of LV Diastolic FillingNicoleNo ratings yet
- RUNDOWN West Borneo Cardiovascular Annual Meeting (WeBCAM) 2023Document3 pagesRUNDOWN West Borneo Cardiovascular Annual Meeting (WeBCAM) 2023Bayu Zeva WirasaktiNo ratings yet
- ECG NotesDocument7 pagesECG NotesShams NabeelNo ratings yet
- Pengaruh Kompresi RJP Dengan Metronom Terhadap Kualitas Kompresi RJP Yang Dilakukan Mahasiswa PerawatDocument7 pagesPengaruh Kompresi RJP Dengan Metronom Terhadap Kualitas Kompresi RJP Yang Dilakukan Mahasiswa PerawatGabriela Adeleda LeiwakabessyNo ratings yet
- For More Free Medical Powerpoint Presentations Visit WebsiteDocument24 pagesFor More Free Medical Powerpoint Presentations Visit Websitevanstar7No ratings yet
- ECG To Localize VADocument48 pagesECG To Localize VAnadia shabriNo ratings yet
- Classification of MurmursDocument2 pagesClassification of MurmursNazneen SiddiquiNo ratings yet
- UntitledDocument135 pagesUntitledDr.younes95 RekaaneyNo ratings yet
- Ventricular Arrhythmia - VT: Braghmandaru A.BDocument113 pagesVentricular Arrhythmia - VT: Braghmandaru A.BFaisol SiddiqNo ratings yet
- Rheumatic Heart Disease Short Case PresentationDocument1 pageRheumatic Heart Disease Short Case PresentationPrerna SehgalNo ratings yet
- Annotated Final Exam Answers: Ashi AclsDocument7 pagesAnnotated Final Exam Answers: Ashi AclsLisete NunesNo ratings yet
- Huszar's Basic Dysrhythmias and Acute Coronary Syndromes: Interpretation and Management Text & Pocket Guide Package - Ebook Keith WesleyDocument54 pagesHuszar's Basic Dysrhythmias and Acute Coronary Syndromes: Interpretation and Management Text & Pocket Guide Package - Ebook Keith Wesleyrichard.knapp379100% (1)
- Med II-LE1-1.03 Arrhythmia NotesDocument14 pagesMed II-LE1-1.03 Arrhythmia NotesAbigael SantosNo ratings yet
- Wolff-Parkinson-White Syndrome: Anatomy, Epidemiology, Clinical Manifestations, and Diagnosis - UpToDateDocument46 pagesWolff-Parkinson-White Syndrome: Anatomy, Epidemiology, Clinical Manifestations, and Diagnosis - UpToDateKarla ChongNo ratings yet
- CardiomyopathyDocument13 pagesCardiomyopathyRaprnaNo ratings yet
- Soap For Atrial FibrillationDocument6 pagesSoap For Atrial FibrillationSombolayuk PriskaNo ratings yet
- Konsep Dasar EKGDocument58 pagesKonsep Dasar EKGBoby GeaNo ratings yet
- Dressler's Syndrome Case ReportDocument3 pagesDressler's Syndrome Case ReportResearch ParkNo ratings yet
- 118 Skills Lab-Week 2-ECG TakingDocument8 pages118 Skills Lab-Week 2-ECG TakingKeisha BartolataNo ratings yet
- High Current Vs High Energy BiphasicDocument4 pagesHigh Current Vs High Energy BiphasicPT. Aedindo Lintas LestariNo ratings yet
- CARDIO PPT Diastolic MurmursDocument47 pagesCARDIO PPT Diastolic MurmursHenry Franz Flores NicolásNo ratings yet
- Tachycardia Complicated by Bradycardia Then Another Form of TachycardiaDocument7 pagesTachycardia Complicated by Bradycardia Then Another Form of TachycardiaLam Sin WingNo ratings yet