You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Maintenance Guide PDFDocument2 pagesMaintenance Guide PDFRosarioBengocheaSecoNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Early Warning SignsDocument1 pageEarly Warning SignsRosarioBengocheaSecoNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- ConnectednessDocument13 pagesConnectednessRosarioBengocheaSeco100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- ConnectednessDocument13 pagesConnectednessRosarioBengocheaSeco100% (1)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Activities For Assessing and Developing ReadinessDocument17 pagesActivities For Assessing and Developing ReadinessRosarioBengocheaSecoNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Bell 2010Document8 pagesBell 2010RosarioBengocheaSecoNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Vaskin 2009Document3 pagesVaskin 2009RosarioBengocheaSecoNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Couture 2006Document20 pagesCouture 2006RosarioBengocheaSecoNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Psychiatry Research: Philip Brittain, Dominic H. Ffytche, Allison Mckendrick, Simon SurguladzeDocument6 pagesPsychiatry Research: Philip Brittain, Dominic H. Ffytche, Allison Mckendrick, Simon SurguladzeRosarioBengocheaSecoNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Ziv 2011Document2 pagesZiv 2011RosarioBengocheaSecoNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Social Perception and Social Skill in SchizophreniaDocument12 pagesSocial Perception and Social Skill in SchizophreniaRosarioBengocheaSecoNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Social Cognition in Schizophrenia, Part 2: 12-Month Stability and Prediction of Functional Outcome in First-Episode PatientsDocument8 pagesSocial Cognition in Schizophrenia, Part 2: 12-Month Stability and Prediction of Functional Outcome in First-Episode PatientsRosarioBengocheaSecoNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Roberts 2009Document7 pagesRoberts 2009RosarioBengocheaSecoNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- PRF CGF AFG PRP PRGF and Sticky Bone or I-PRF - Bauer SmilesDocument1 pagePRF CGF AFG PRP PRGF and Sticky Bone or I-PRF - Bauer SmilesArmareality ArmarealityNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Early Warning ScoresDocument14 pagesEarly Warning ScoresmuchtarNo ratings yet
- Medication To Manage Abortion and MiscarriageDocument8 pagesMedication To Manage Abortion and MiscarriageNisaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Use of A Modified Matrix Band Technique To Restore Subgingival Root CariesDocument6 pagesUse of A Modified Matrix Band Technique To Restore Subgingival Root CariesDina NovaniaNo ratings yet
- Jan Feb 2024Document124 pagesJan Feb 2024Gerardo Valenzuela GonzálezNo ratings yet
- Tariffs Operation Manual v22Document147 pagesTariffs Operation Manual v22Nanayaw CasperNo ratings yet
- Technical University of Kenya: Orientation Programme For First Year Students 2020/2021Document5 pagesTechnical University of Kenya: Orientation Programme For First Year Students 2020/2021Samuel MwangiNo ratings yet
- Dr. Archya Sengupta: ContactDocument2 pagesDr. Archya Sengupta: ContactJenefer AntoNo ratings yet
- Scope of Nle1113Document379 pagesScope of Nle1113ericNo ratings yet
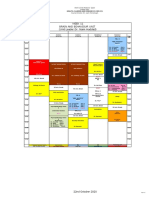
- Week 11 Brain and Behaviour Unit (Unit Leader:Dr. Naim Haddad)Document1 pageWeek 11 Brain and Behaviour Unit (Unit Leader:Dr. Naim Haddad)f3er3No ratings yet
- PHIN LectureDocument13 pagesPHIN Lecturedanilotinio2No ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Factors To Consider in Hospital Design and Construction: Home Services AboutDocument17 pagesFactors To Consider in Hospital Design and Construction: Home Services AboutDanaya AstreroNo ratings yet
- Pain Management Opioids SummariesDocument55 pagesPain Management Opioids SummariesPeter KhanhNo ratings yet
- 9 Department of Health - Diabetes Mellitus Prevention and Control Program - 2011-12-23Document2 pages9 Department of Health - Diabetes Mellitus Prevention and Control Program - 2011-12-23Evelyn Chu Nevado67% (3)
- List of Maxicare Prepaid Products: Maxicare Eready - The Pre-Paid Maxicare Card Which Covers Emergency-RelatedDocument6 pagesList of Maxicare Prepaid Products: Maxicare Eready - The Pre-Paid Maxicare Card Which Covers Emergency-Relatedarellano lawschoolNo ratings yet
- Informative Essay On Drug AddictionDocument2 pagesInformative Essay On Drug AddictionKhaing2673% (15)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Dental Fear and Concomitant Factors in 3-6 Year-Old ChildrenDocument5 pagesDental Fear and Concomitant Factors in 3-6 Year-Old ChildrenDrSugandh MittalNo ratings yet
- CD011145 Pub2Document185 pagesCD011145 Pub2Guilherme RodriguesNo ratings yet
- PJN Jul-Dec 2019 Complete v1 PDFDocument62 pagesPJN Jul-Dec 2019 Complete v1 PDFIsabel Bibat DavidNo ratings yet
- Reverie Psychedelics and Indiana Health Group Partner To Develop World-Class Psychedelic Research CenterDocument3 pagesReverie Psychedelics and Indiana Health Group Partner To Develop World-Class Psychedelic Research CenterPR.comNo ratings yet
- Stages of Hospital DevelopmentDocument16 pagesStages of Hospital Developmentstanis555100% (1)
- RN - Er Application PacketDocument56 pagesRN - Er Application PacketJohnny Gto0% (1)
- Good Manufacturing Practice (GMP)Document2 pagesGood Manufacturing Practice (GMP)Shailesh GuptaNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Comparison of The Efficacy and Safety of GlimepiriDocument6 pagesComparison of The Efficacy and Safety of GlimepirinnNo ratings yet
- Safe Motherhood PDFDocument13 pagesSafe Motherhood PDFcarissa rhezaNo ratings yet
- CMVDocument24 pagesCMVecko Roman100% (1)
- 2008 SPRING AnesthNewsDocument31 pages2008 SPRING AnesthNewsDev RaiNo ratings yet
- CBL For UrologyDocument2 pagesCBL For UrologyMin Phone Thant AungNo ratings yet
- Tribhuvan University Teaching Hospital PDFDocument4 pagesTribhuvan University Teaching Hospital PDFashqNo ratings yet
- Dr. Lucky Saputra, SP - KJ (K), M.Kes-Schizophrenia and SexualityDocument16 pagesDr. Lucky Saputra, SP - KJ (K), M.Kes-Schizophrenia and SexualityKorn IbraNo ratings yet
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)