Professional Documents
Culture Documents
A Practical Guide To Clinical Medicine-Neurology PDF
Uploaded by
Iustitia Septuaginta SambenOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
A Practical Guide To Clinical Medicine-Neurology PDF
Uploaded by
Iustitia Septuaginta SambenCopyright:
Available Formats
9/12/2016
APracticalGuidetoClinicalMedicine
APracticalGuidetoClinicalMedicine
A comprehensive physical examination and clinical education site for medical
students and other health care professionals
Web Site Design by Jan Thompson, Program Representative, UCSD School of Medicine.
Content and Photographs by Charlie Goldberg, M.D., UCSD School of Medicine and VA
Medical Center, San Diego, California 920930611.
Send Comments to: Charlie Goldberg, M.D.
Introduction
HistoryofPresentIllness
TheRestoftheHistory
ReviewofSystems
VitalSigns
TheEyeExam
HeadandNeckExam
TheLungExam
CardiovascularExam
ExamoftheAbdomen
BreastExam
MaleGenital/RectalExam
TheUpperExtremities
TheLowerExtremities
MusculoSkeletalExam
TheMentalStatusExam
TheNeurologicalExam
PhysicalExamCheckLists
MedicalLinks
WriteUps
TheOralPresentation
OutpatientClinics
InpatientMedicine
ClinicalDecisionMaking
PhysicalExamLectureSeries
AFewThoughts
CommonlyUsedAbbreviations
References
The"daVinciAnatomyIcon"denotesalinktorelatedgrossanatomypictures.
TheNeurologicalExamination
Cranial
Nerves
SensoryandMotor
Examinations
Reflex
Testing
Coordination
Gait
Testing
MakingSenseof
Neurological
Findings
Introduction
Thegoalsoftheneurologicalexaminationareseveral:
1.Forpatientspresentingwithsymptomssuggestiveofaneurologicalproblem,theexaminationshould:
a.Determine,onthebasisofanorganizedandthoroughexamination,whetherinfactneurological
dysfunctionexists.
b.Identifywhichcomponent(s)oftheneurologicalsystemareaffected(e.g.motor,sensory,cranial
nerves,orpossiblyseveralsystemssimultaneously).
c.Ifpossible,determinethepreciselocationoftheproblem(e.g.peripheralvcentralnervoussystem
regionandsideofthebrainaffectedetc.).
d.Onthebasisofthesefindings,generatealistofpossibleetiologies.Unlikelydiagnosescanbe
excludedandappropriatetesting(e.g.brainandspinalcordimaging)thenappliedinanorderlyand
logicalfashion.
2.Screeningforthepresenceofdiscreteabnormalitiesinpatientsatriskforthedevelopmentofneurological
disorders.Thisisappropriateforindividualswhohavenoparticularsubjectivesymptomssuggestiveofa
neurologicalproblem,yethavesystemicillnessesthatmightputthematriskforsubtledysfunction.
Diabeticpatients,forexample(particularlythosewithlongstandingpoorcontrol),maydevelop
https://meded.ucsd.edu/clinicalmed/neuro2.htm
1/40
9/12/2016
APracticalGuidetoClinicalMedicine
peripheralnervedysfunction.Thismayonlybedetectedthroughcarefulsensorytesting(seebelowunder
SensoryTesting),whichwouldhaveimportantclinicalimplications.
3.Cursoryscreening/documentationofbaselinefunctionforthosewhoareotherwisehealthy.Inpatients
withneithersignsnorriskfactorsforneurologicaldisease,it'sunlikelythatthedetailedexamwould
uncoveroccultproblems.SimplyobservingthepatientduringthecourseoftheusualH&P(i.e.watching
themwalk,getupanddownfromtheexamtable,etc.)maywellsuffice.Manyexaminersincorporate
someaspectsoftheneuroexamintotheirstandardevaluations.CranialNervetesting,forexample,canbe
easilyblendedintotheHeadandNeckevaluation.Decidingwhatotheraspectstoroutinelyincludeis
basedonjudgmentandexperience.
Themajorareasoftheexam,coveringthemosttestablecomponentsoftheneurologicalsystem,include:
1.Mentalstatustesting(coveredinaseparatesectionofthiswebsite)
2.CranialNerves
3.Musclestrength,toneandbulk
4.Reflexes
5.Coordination
6.SensoryFunction
7.Gait
Realandimaginedproblemswiththeneurologicalexamination:
Theneurologicalexaminationisoneoftheleastpopularand(perhaps)mostpoorlyperformedaspectsofthe
completephysical.Isuspectthatthissituationexistsforseveralreasons:
1.Thisexamisperceivedasbeingtimeandlaborintensive.
2.Studentsandhousestaffneverdevelopanadequatelevelofconfidenceintheirabilitytoperformthe
exam,norintheaccuracyoftheirfindings.This,inturn,probablytranslatesintopoorperformancelater
intheircareers.
3.Examfindingsareoftenquitesubjective.Thus,particularlywhentheexaminerdoesnothaveconfidence
intheirabilities(seeabove),interpretationoftheresultscanbeproblematic.
4.Understanding/Interpretationofsomeneurologicalfindingsrequiresanindepthunderstandingof
neuroanatomyandpathophysiology.Asmanycliniciansdonotseealargenumberofpatientswith
neurologicaldisorders,theylikelymaintainalimitedworkingunderstandingofthisinformation.
5.Thereisanoverrelianceontheutilityofneuroimaging(e.g.CT,MRI).Thesestudiesprovidean
evaluationofanatomybutnotfunction.Thus,whileextremelyhelpful,theymustbeinterpretedwithinthe
contextofexamfindings.Carefulexaminationmaymakeimagingunnecessary.Also,examfindingscan
makeastrongcaseforthepresenceofapathologicprocess,evenifitisnotseenonaparticular
radiologicalstudy(i.e.therearelimitstowhatcanbeseenoneventhemosthightechimaging).
Theabovearenotmeanttolowerexpectationswithregardstohowwellaphysicianshouldbeexpectedtolearn
andperformtheneurologicalexamination.Rather,Imentionthesepointstohighlightsomeoftherealand
imaginedobstaclestoclinicalperformance.Likeallotheraspectsofthephysicalexam,thereisawealthof
informationthatcanbeobtainedfromtheneurologicalexamination,providedthatitisdonecarefullyand
accurately.Thisis,ofcourse,predicatedonlearninghowtodoitcorrectly.Afewpractical
considerations/suggestions:
1.Ingeneral,theneurologicalexaminationisnotappliedinitsentiretytoasymptomatic,otherwisehealthy
peopleastheyield(i.e.likelihoodofidentifyingoccultdisease)wouldbequitelow.Itis,however,agood
ideatopracticetheexamearlyinyourcareers,evenwhenworkingwithnormalpatients.Thiswill
improvethefacilitywithwhichyouperformtheexam,provideyouwithabettersenseoftherangeof
normal,increasetheaccuracyoftheresultsgenerated,andgiveyouconfidenceinthemeaningoffindings
identifiedwhenevaluatingotherpatients.
https://meded.ucsd.edu/clinicalmed/neuro2.htm
2/40
9/12/2016
APracticalGuidetoClinicalMedicine
2.Itissometimesappropriatetoperformonlycertainpartsoftheneurologicalexamination(e.g.justcranial
nervesoronlymotortesting)Thesesituationswillbecomeapparentwithexperience.
3.Thetestingdescribedbelowisstillratherbasic.Therearemanyadditionalaspectsoftheexamthatshould
beappliedinspecificsettings.Theyarebeyondthescopeofthistext,butcanbefoundinother
references.
4.Takeadvantageofthoseopportunitieswhenamoreexperiencedclinicianexaminesoneofyourpatients.
Whenpossible,watchthemperformtheirexam.Thengobackaloneandverifythefindings.
Likeanyotheraspectoftheexam,theneurologicalassessmenthaslimits.Testingofonesystemisoften
predicatedonthenormalfunctionofotherorgansystems.If,forexample,apatientisvisuallyimpaired,they
maynotbeabletoperformfingertonosetesting,apartoftheassessmentofcerebellarfunction(seebelow).Or,
apatient'sseveredegenerativehipdiseasewillpreventthemfromwalking,makingthataspectoftheexam
impossibletoassess.Theinterpretationof"findings"mustthereforetakethesethingsintoaccount.Onlyinthis
waycanyougenerateanaccuratepicture.Doingthis,ofcourse,takespracticeandexperience.
CranialNerve(CN)Testing
CN2
CN3,4,6
CN5
CN7
CN8
CN9,10
CN11
CN12
Manypractitionersincorporatecranialnervetestingwiththeircompleteexaminationoftheheadandneck(see
theHeadandNecksectionofthiswebsitefordetails).AdetaileddescriptionoftheCNassessmentisprovided
below.Aseachhalfofthebodyhasitsowncranialnerve,bothrightandleftsidesmustbechecked
independently.
CranialNerve1(Olfactory):Formalassessmentofabilitytosmellisgenerallyomitted,unlessthereisaspecific
complaint.Ifitistobetested:
1.1.Checktomakesurethatthepatientisabletoinhaleandexhalethroughtheopennostril.
2.Havethepatientclosetheireyes.
3.Presentasmalltesttubefilledwithsomethingthathasadistinct,commonodor(e.g.groundcoffee)tothe
opennostrils.Thepatientshouldbeabletocorrectlyidentifytheodoratapproximately10cm.
FormoreinformationaboutCN1,seethefollowinglinks:
YaleUniversityCranialNerveReviewSite
UniformServicesSchoolofMedicineCranialNerveReviewSite
CranialNerve2(Optic):Thisnervecarriesvisualimpulsesfromtheeyetotheopticalcortexofthebrainby
meansoftheoptictracts.Testinginvolves3phases(alsocoveredinthesectionofthissitededicatedtotheEye
Exam):
1.Acuity:
a.Eacheyeistestedseparately.Ifthepatientusesglassestoviewdistantobjects,theyshouldbe
permittedtowearthem(referredtoasbestcorrectedvision).
b.ASnellenChartisthestandard,wallmounteddeviceusedforthisassessment.Patientsareaskedto
readthelettersornumbersonsuccessivelylowerlines(eachwithsmallerimages)untilyouidentify
thelastlinewhichcanbereadwith100%accuracy.Eachlinehasafractionwrittennexttoit.20/20
indicatesnormalvision.20/400meansthatthepatient'svision20feetfromanobjectisequivalent
tothatofanormalpersonviewingthesameobjectfrom400feet.Inotherwords,thelargerthe
denominator,theworsethevision.
https://meded.ucsd.edu/clinicalmed/neuro2.htm
3/40
9/12/2016
APracticalGuidetoClinicalMedicine
Snellenchartformeasuringvisualacuity
c.TherearehandheldcardsthatlooklikeSnellenChartsbutarepositioned14inchesfromthe
patient.Theseareusedsimplyforconvenience.Testingandinterpretationareasdescribedforthe
Snellen.
Handheldvisualacuitycard
d.Ifneitherchartisavailableandthepatienthasvisualcomplaints,someattemptshouldbemadeto
objectivelymeasurevisualacuity.Thisisacriticallyimportantreferencepoint,particularlywhen
tryingtocommunicatethemagnitudeofavisualdisturbancetoaconsultingphysician.Canthe
patientreadnewsprint?Theheadlineofanewspaper?Distinguishfingersorhandmovementin
frontoftheirface?Detectlight?Failureateachlevelcorrelateswithamoresevereproblem.
https://meded.ucsd.edu/clinicalmed/neuro2.htm
4/40
9/12/2016
APracticalGuidetoClinicalMedicine
2.VisualFieldTesting:Specificareasoftheretinareceiveinputfrompreciseareasofthevisualfield.This
informationiscarriedtothebrainalongwelldefinedanatomicpathways.Holesinvision(referredtoas
visualfieldcuts)arecausedbyadisruptionalonganypointinthepathfromtheeyeballtothevisual
cortexofthebrain.Visualfieldscanbecrudelyassessedasfollows:
a.Theexaminershouldbenosetonosewiththepatient,separatedbyapproximately8to12inches.
b.Eacheyeischeckedseparately.Theexaminerclosesoneeyeandthepatientclosestheone
opposite.Theopeneyesshouldthenbestaringdirectlyatoneanother.
c.Theexaminershouldmovetheirhandouttowardstheperipheryofhis/hervisualfieldontheside
wheretheeyesareopen.Thefingershouldbeequidistantfrombothpersons.
d.Theexaminershouldthenmovethewigglingfingerintowardsthem,alonganimaginaryline
drawnbetweenthetwopersons.Thepatientandexaminershoulddetectthefingeratmoreorless
thesametime.
e.Thefingeristhenmovedouttothediagonalcornersofthefieldandmovedinwardsfromeachof
thesedirections.Testingisthendonestartingatapointinfrontoftheclosedeyes.Thewiggling
fingerismovedtowardstheopeneyes.
f.Theothereyeisthentested.
Meaningfulinterpretationispredicatedupontheexaminerhavingnormalfields,astheyareusing
themselvesforcomparison.
Iftheexaminercannotseemtomovetheirfingertoapointthatisoutsidethepatient'sfielddon't
worry,asitsimplymeansthattheirfieldsarenormal.
Interpretation:Thistestisrathercrude,anditisquitepossibletohavesmallvisualfielddefectsthat
wouldnotbeapparentonthistypeoftesting.Priortointerpretingabnormalfindings,theexaminer
mustunderstandthenormalpathwaysbywhichvisualimpulsestravelfromtheeyetothebrain.
Formoreinformationaboutvisualfieldtesting,seethefollowinglinks:
WashingtonUniversity,reviewofvisualfieldoftestingandpathology
UniversityofArkansas,grossanatomyofvisualpathway
3.Pupils:Thepupilhasafferent(sensory)nervesthattravelwithCN2.Thesenervescarrytheimpulse
generatedbythelightbacktowardsthebrain.Theyfunctioninconcertwithefferent(motor)nervesthat
travelwithCN3andcausepupillaryconstriction.SeenunderCN3forspecificsoftesting.
FormoreinformationaboutCN2,seethefollowinglinks:
YaleUniversityCranialNerveReviewSite
UniformServicesSchoolofMedicineCranialNerveReviewSite
Cranialnerves3,4and6&extraocularmovements:
Normally,theeyesmoveinconcert(iewhenlefteyemovesleft,righteyemovesinsamedirectiontoasimilar
degree).Thebraintakestheinputfromeacheyeandputsittogethertoformasingleimage.Thiscoordinated
movementdependson6extraocularmusclesthatinsertaroundtheeyeballsandallowthemtomoveinall
directions.Eachmuscleisinnervatedbyoneof3CranialNerves(CNs):CNs3,4and6.Movementsare
describedas:elevation(pupildirectedupwards),depression(pupildirecteddownwards),adbduction(pupil
directedlaterally),adduction(pupildirectedmedially),extorsion(topofeyerotatingawayfromthenose),and
intorsion(topofeyerotatingtowardsthenose).
https://meded.ucsd.edu/clinicalmed/neuro2.htm
5/40
9/12/2016
APracticalGuidetoClinicalMedicine
The3CNsresponsibleforeyemovementandthemusclesthattheycontrolareasfollows:
CN4(Trochlear):ControlstheSuperiorObliquemuscle.
CN6(Abducens):ControlstheLateralRectusmuscle.
CN3(Oculomotor):Controlstheremaining4muscles(inferioroblique,inferiorrectus,superiorrectus,and
medialrectus).CN3alsoraisestheeyelidandmediatesconstrictionofthepupil(discussedbelow).
Themnemonic"SO4,LR6,AllTheRest3"mayhelpremindyouwhichCNdoeswhat(SuperiorObliqueCN
4,LateralRectusCN6,AllTheRestofthemusclesinnervatedbyCN3).
EOMsandtheirfunction:
Themedialandlateralrectusmusclesaredescribedfirst,astheirfunctionsareverystraightforward:
Lateralrectus:Abduction(ielateralmovementalongthehorizontalplane)
Medialrectus:Adduction(ie.Medialmovementalongthehorizontalplane)
Theremainingmuscleseachcausesmovementinmorethanonedirection(e.g.somecombinationof
elevation/depression,abduction/adduction,intorsion/extorsion).Thisisduetothefactthattheyinsertonthe
eyeballatvariousangles,andinthecaseofthesuperioroblique,thruapulley.Reviewoftheoriginand
insertionofeachmuscleshedslightonitsactions(seelinks@theendofthissection).Thenetimpactofany
oneEOMistheresultofthepositionoftheeyeandthesumofforcesfromallothercontributingmuscles.
SpecificactionsoftheremainingEOMsaredescribedbelow.Theactionwhichthemuscleprimarilyperformsis
listedfirst,followedbysecondaryandthentertiaryactions.
Inferiorrectus:depression,extorsionandadduction.
Superiorrectus:elevation,intorsionandadduction
Superioroblique:intorsion,depressionandabduction
Inferioroblique:extorsion,elevationandabduction
https://meded.ucsd.edu/clinicalmed/neuro2.htm
6/40
9/12/2016
APracticalGuidetoClinicalMedicine
Practicallyspeaking,cranialnervetestingisdonesuchthattheexaminercanobserveeyemovementsinall
directions.Themovementsshouldbesmoothandcoordinated.Toassess,proceedasfollows:
1.Standinfrontofthepatient.
2.Askthemtofollowyourfingerwiththeireyeswhilekeepingtheirheadinoneposition
3.Usingyourfinger,traceanimaginary"H"orrectangularshapeinfrontofthem,makingsurethatyour
fingermovesfarenoughoutandupsothatyou'reabletoseeallappropriateeyemovements(ielateraland
up,lateraldown,medialdown,medialup).
4.Attheend,bringyourfingerdirectlyintowardsthepatient'snose.Thiswillcausethepatienttolook
crosseyedandthepupilsshouldconstrict,aresponsereferredtoasaccommodation.
TestingExtraocularMovements
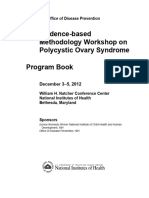
Pathology:Isolatedlesionsofacranialnerveorthemuscleitselfcanadverselyaffectextraocularmovement.
Patientswillreportdiplopia(doublevision)whentheylookinadirectionthat'saffected.Thisisbecausethe
braincan'tputtogetherthediscordantimagesinawaythatformsasinglepicture.Inresponse,theywilleither
assumeaheadtiltthatattemptstocorrectfortheabnormaleyepositioningorclosetheabnormaleye.Asan
example,thepatientshownbelowhasaleftcranialnerve6lesion,whichmeansthathisleftlateralrectusno
longerfunctions.Whenhelooksright,hisvisionisnormal.However,whenhelooksleft,heexperiencesdouble
visionasthelefteyecan'tmovelaterally.Thisisreferredtoashorizontaldiplopia.
https://meded.ucsd.edu/clinicalmed/neuro2.htm
7/40
9/12/2016
APracticalGuidetoClinicalMedicine
LeftCN6Palsy
Patientwasaskedtolookleft.Notethatlefteyewillnotabduct.
It'sworthmentioningthatdisordersoftheextraocularmusclesthemselves(andnottheCNwhichinnervate
them)canalsoleadtoimpairedeyemovement.Forexample,picturedbelowisapatientwhohassuffereda
traumaticleftorbitalinjury.Theinferiorrectusmusclehasbecomeentrappedwithintheresultingfracture,
preventingthelefteyefrombeingabletolookdownward.Thescleralbloodandperiorbitalechymosisare
secondarytothetraumaaswell.
*FormoreonEOMsgoto:EyesEOMshttp://meded.ucsd.edu/clinicalmed/eyes.htm#Extra
Asmentionedabove,CN3alsoinnervatesthemusclewhichraisestheuppereyelid(LevatorPalpebrae
Superiorismuscle).Thiscanbeassessedbysimplylookingatthepatient.IfthereisCN3dysfunction,the
eyelidonthatsidewillcovermoreoftheiriscomparedwiththeothereye.Thisisreferredtoasptosis.
RighteyeptosisfromCN3Palsy.Inaddition,therighteyeisdirectedlaterally,whichisduetounopposed
effectsofCNs4&6.Thedilatedrightpupilisexplainedbelow.
Theresponseofpupilstolightiscontrolledbyafferent(sensory)nervesthattravelwithCN2andefferent
(motor)nervesthattravelwithCN3.Theseinnervatetheciliarymuscle,whichcontrolsthesizeofthepupil.
Testingisperformedasfollows:
https://meded.ucsd.edu/clinicalmed/neuro2.htm
8/40
9/12/2016
APracticalGuidetoClinicalMedicine
1.Ithelpsiftheroomisabitdim,asthiswillcausethepupiltobecomemoredilated.
2.Usinganylightsource(flashlight,otoophtahlmoscope,etc),shinethelightintooneeye.Thiswillcause
thatpupiltoconstrict,referredtoasthedirectresponse.
3.Removethelightandthenreexposeittothesameeye,thoughthistimeobservetheotherpupil.Itshould
alsoconstrict,referredtoastheconsensualresponse.Thisoccursbecauseafferentimpulsesfromoneeye
generateanefferentresponse(i.e.signaltoconstrict)thatissenttobothpupils.
4.Ifthepatient'spupilsaresmallatbaselineoryouareotherwisehavingdifficultyseeingthechanges,take
yourfreehandandplaceitabovetheeyessoastoprovidesomeshade.Thisshouldcausethepupilsto
dilateadditionally,makingthechangewhentheyareexposedtolightmoredramatic.Ifyouarestill
unabletoappreciatearesponse,askthepatienttoclosetheireye,generatingmaximumdarknessandthus
dilatation.Thenaskthepatienttoopentheeyeandimmediatelyexposeittothelight.Thiswill
(hopefully)makethechangefromdilatedtoconstrictedveryapparent.
Interpretation:
1.Undernormalconditions,bothpupilswillappearsymmetric.Directandconsensualresponseshouldbe
equalforboth.
2.Asymmetryofthepupilsisreferredtoasaniosocoria.Somepeoplewithanisocoriahavenounderlying
neuropathology.Inthissetting,theasymmetrywillhavebeenpresentforalongtimewithoutchangeand
thepatientwillhavenootherneurologicalsignsorsymptoms.Thedirectandconsensualresponsesshould
bepreserved.
3.Anumberofconditionscanalsoaffectthesizeofthepupils.Medications/intoxicationswhichcause
generalizedsympatheticactivationwillresultindilatationofbothpupils.Otherdrugs(e.g.narcotics)
causesymmetricconstrictionofthepupils.Thesefindingscanprovideimportantclueswhendealingwith
anagitatedorcomatosepatientsufferingfrommedicationoverdose.Eyedropsknownasmydriaticagents
areusedtoparalyzethemuscles,resultingmarkeddilatationofthepupils.Theyareusedduringadetailed
eyeexamination,allowingaclearviewoftheretina.Addiitonally,anyprocesswhichcausesincreased
intracranialpressurecanresultinadilatedpupilthatdoesnotrespondtolight.
4.Iftheafferentnerveisnotworking,neitherpupilwillrespondwhenlightisshinedintheaffectedeye.
Lightshinedinthenormaleye,however,willcausetheaffectedpupiltoconstrict.That'sbecausethe
efferent(signaltoconstrict)responseinthiscaseisgeneratedbytheafferentimpulsereceivedbythe
normallyfunctioningeye.Thisisreferredtoasanafferentpupildefect.
5.Iftheefferentnerveisnotworking,thepupilwillappeardilatedatbaselineandwillhaveneitherdirect
norconsensualpupillaryresponses.
RightCN3PalsyNotethattherightpupilisdilatedrelativetotheleft,duetolossofefferent
https://meded.ucsd.edu/clinicalmed/neuro2.htm
9/40
9/12/2016
APracticalGuidetoClinicalMedicine
input.Theptosisandabnormaleyepositioningarediscussedabove.
FormoreinformationaboutpupillaryresponseandCN3,seethefollowinglinks:
MoreonExtraocularmovements:http://www.tedmontgomery.com/the_eye/eom.html#top
DartmouthNeurosciencesExtraocularmovements
http://www.dartmouth.edu/~dons/part_1/chapter_4.html
YaleUniversityExtraocularMuscleshttp://info.med.yale.edu/caim/cnerves/cn3/cn3_3.html
YaleUniversityCranialNerveReviewSite
UCDavisExtraOccularMovementandPupilaryResponseSimulator
CN4(Trochlear):SeenunderCN3.
CN5(Trigeminal):Thisnervehasbothmotorandsensorycomponents.
AssessmentofCN5SensoryFunction:Thesensorylimbhas3majorbranches,eachcoveringroughly1/3ofthe
face.Theyare:theOphthlamic,Maxillary,andMandibular.Assessmentisperformedasfollows:
1.Useasharpimplement(e.g.brokenwoodenhandleofacottontippedapplicator).
2.Askthepatienttoclosetheireyessothattheyreceivenovisualcues.
3.Touchthesharptipofthesticktotherightandleftsideoftheforehead,assessingtheOphthalmicbranch.
4.Touchthetiptotherightandleftsideofthecheekarea,assessingtheMaxillarybranch.
5.Touchthetiptotherightandleftsideofthejawarea,assessingtheMandibularbranch.
Thepatientshouldbeabletoclearlyidentifywhenthesharpendtouchestheirface.Ofcourse,makesurethat
youdonotpushtoohardasthefaceisnormallyquitesensitive.TheOphthalmicbranchofCN5alsoreceives
sensoryinputfromthesurfaceoftheeye.Toassessthiscomponent:
1.Pulloutawispofcotton.
2.Whilethepatientislookingstraightahead,gentlybrushthewispagainstthelateralaspectofthesclera
(outerwhiteareaoftheeyeball).
3.Thisshouldcausethepatienttoblink.BlinkingalsorequiresthatCN7functionnormally,asitcontrols
eyelidclosure.
AssessmentofCN5MotorFunction:ThemotorlimbofCN5innervatestheTemporalisandMassetermuscles,
bothimportantforclosingthejaw.Assessmentisperformedasfollows:
1.PlaceyourhandonbothTemporalismuscles,locatedonthelateralaspectsoftheforehead.
2.Askthepatienttotightlyclosetheirjaw,causingthemusclesbeneathyourfingerstobecometaught.
3.ThenplaceyourhandsonbothMassetermuscles,locatedjustinfromoftheTemperoMandibularjoints
(pointwherelowerjawarticulateswithskull).
https://meded.ucsd.edu/clinicalmed/neuro2.htm
10/40
9/12/2016
APracticalGuidetoClinicalMedicine
4.Askthepatienttotightlyclosetheirjaw,whichshouldagaincausethemusclesbeneathyourfingersto
becometaught.Thenaskthemtomovetheirjawfromsidetoside,anotherfunctionoftheMassester.
FormoreinformationaboutCN5motorfunction,seethefollowinglinks:
YaleUniversityCranialNerveReviewSite
UniformServicesSchoolofMedicineCranialNerveReviewSite
CN6(Abducens):SeeunderCN3.
CN7(Facial):Thisnerveinnervatesmanyofthemusclesoffacialexpression.Assessmentisperformedas
follows:
1.Firstlookatthepatient'sface.Itshouldappearsymmetric.Thatis:
a.Thereshouldbethesameamountofwrinklesapparentoneithersideoftheforehead...barring
asymmetricBoToxinjection!
b.Thenasolabialfolds(linescomingdownfromeithersideofthenosetowardsthecornersofthe
mouth)shouldbeequal
c.Thecornersofthemouthshouldbeatthesameheight
Ifthereisanyquestionastowhetheranapparentasymmetryifneworold,askthepatientforapicture
(oftenfoundonadriver'slicense)forcomparison.
2.Askthepatienttowrinkletheireyebrowsandthenclosetheireyestightly.CN7controlsthemusclesthat
closetheeyelids(asopposedtoCN3,whichcontrolsthemuscleswhichopenthelid).Youshouldnotbe
abletoopenthepatient'seyelidswiththeapplicationofgentleupwardspressure.
3.Askthepatienttosmile.Thecornersofthemouthshouldrisetothesameheightandequalamountsof
teethshouldbevisibleoneitherside.
4.Askthepatienttopuffouttheircheeks.Bothsidesshouldpuffequallyandairshouldnotleakfromthe
mouth.
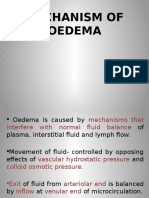
Interpretation:CN7hasaprecisepatternofinervation,whichhasimportantclinicalimplications.Therightand
leftuppermotorneurons(UMNs)eachinnervateboththerightandleftlowermotorneurons(LMNs)thatallow
https://meded.ucsd.edu/clinicalmed/neuro2.htm
11/40
9/12/2016
APracticalGuidetoClinicalMedicine
theforeheadtomoveupanddown.However,theLMNsthatcontrolthemusclesofthelowerfaceareonly
innervatedbytheUMNfromtheoppositesideoftheface.
CN7FacialNerve
PrecisePatternofInnervation
Thus,inthesettingofCN7dysfunction,thepatternofweaknessorparalysisobservedwilldifferdependingon
whethertheUMNorLMNisaffected.Specifically:
1.UMNdysfunction:Thismightoccurwithacentralnervoussystemevent,suchasastroke.Inthesetting
ofRUMNCN7dysfunction,thepatientwouldbeabletowrinkletheirforeheadonbothsidesoftheir
face,astheleftCN7UMNcrossinnervatestheRCN7LMNthatcontrolsthismovement.However,the
patientwouldbeunabletoeffectivelyclosetheirlefteyeorraisetheleftcorneroftheirmouth.
https://meded.ucsd.edu/clinicalmed/neuro2.htm
12/40
9/12/2016
APracticalGuidetoClinicalMedicine
RightcentralCN7dysfunction:Notepreservedabiltiytowrinkleforehead.Leftcornerofmouth,
however,isslightlylowerthanright.Leftnasolabialfoldisslightlylesspronouncedcomparedwithright.
2.LMNdysfunction:ThisoccursmostcommonlyinthesettingofBell'sPalsy,anidiopathic,acuteCN7
peripheralnervepalsy.InthesettingofRCN7peripheral(i.e.LMN)dysfunction,thepatientwouldnot
beabletowrinkletheirforehead,closetheireyeorraisethecorneroftheirmouthontherightside.Left
sidedfunctionwouldbenormal.
LeftperipheralCN7dysfunction:Notelossofforeheadwrinkle,abilitytocloseeye,abilitytoraisecornerof
mouth,anddecreasednasolabialfoldprominenceonleft.
Thisclinicaldistinctionisveryimportant,ascentralvsperipheraldysfunctioncarrydifferentprognosticand
treatmentimplications.Bell'sPalsy(peripheralCN7dysfunction)tendstohappeninpatient'sover50andoften
respondstotreatmentwithAcyclovir(anantiviralagent)andPrednisone(acorticosteroid).Overthecourseof
weeksormonthsthereisusuallyimprovementandoftencompleteresolutionofsymptoms.Assessmentofacute
central(UMN)CN7dysfunctionwouldrequirequiteadifferentapproach(e.g.neuroimagingtodetermine
etiology).
CN7isalsoresponsibleforcarryingtastesensationsfromtheanterior2/3ofthetongue.Howeverasthisis
rarelyofclinicalimport,furtherdiscussionisnotincluded.
FormoreinformationaboutCN7,seethefollowinglinks:
YaleUniversityCranialNerveReviewSite
UniformServicesSchoolofMedicineCranialNerveReviewSite
CN8(Acoustic):CN8carriessoundimpulsesfromthecochleatothebrain.Priortoreachingthecochlea,the
soundmustfirsttraversetheexternalcanalandmiddleear.Auditoryacuitycanbeassessedverycrudelyon
physicalexamasfollows:
1.Standbehindthepatientandaskthemtoclosetheireyes.
2.Whisperafewwordsfromjustbehindoneear.Thepatientshouldbeabletorepeatthesebackaccurately.
Thenperformthesametestfortheotherear.
3.Alternatively,placeyourfingersapproximately5cmfromoneearandrubthemtogether.Thepatient
shouldbeabletohearthesoundgenerated.Repeatfortheotherear.
Formoreinformationaboutearanatomy,seethefollowinglink:
WashingtonUniversityInnerEarAnatomy
Thesetestsarerathercrude.Precisequantification,generallynecessarywheneverthereisasubjectivedeclinein
acuity,requiresspecialequipmentandtraining.
Thecauseofsubjectivehearinglosscanbeassessedwithbedsidetesting.Hearingisbrokeninto2phases:
conductiveandsensorineural.Theconductivephasereferstothepassageofsoundfromtheoutsidetothelevel
https://meded.ucsd.edu/clinicalmed/neuro2.htm
13/40
9/12/2016
APracticalGuidetoClinicalMedicine
ofCN8.Thisincludesthetransmissionofsoundthroughtheexternalcanalandmiddleear.Sensorineuralrefers
tothetransmissionofsoundviaCN8tothebrain.Identificationofconductive(amuchmorecommonproblem
inthegeneralpopulation)defectsisdeterminedasfollows:
WeberTest:
1.Graspthe512Hztuningforkbythestemandstrikeitagainstthebonyedgeofyourpalm,generatinga
continuoustone.Alternativelyyoucangettheforktovibrateby"snapping"theendsbetweenyourthumb
andindexfinger.
512HzTuningFork
2.Holdthestemagainstthepatient'sskull,alonganimaginarylinethatisequidistantfromeitherear.
3.ThebonesoftheskullwillcarrythesoundequallytoboththerightandleftCN8.BothCN8s,inturn,
willtransmittheimpulsetothebrain.
4.Thepatientshouldreportwhetherthesoundwasheardequallyinbothearsorbetterononesidethenthe
other(referredtoaslateralizingtoaside).
WeberTest
https://meded.ucsd.edu/clinicalmed/neuro2.htm
14/40
9/12/2016
APracticalGuidetoClinicalMedicine
RinneTest:
1.Graspthe512Hztuningforkbythestemandstrikeitagainstthebonyedgeofyourpalm,generatinga
continuoustone.
2.Placethestemofthetuningforkonthemastoidbone,thebonyprominencelocatedimmediatelybehind
thelowerpartoftheear.
3.ThevibrationstravelviathebonesoftheskulltoCN8,allowingthepatienttohearthesound.
4.Askthepatienttoinformyouwhentheycannolongerappreciatethesound.Whenthisoccurs,movethe
tuningforksuchthatthetinesareplacedrightnextto(butnottouching)theopeningoftheear.Atthis
point,thepatientshouldbeabletoagainhearthesound.Thisisbecauseairisabetterconductingmedium
thenbone.
RinneTest
Interpretation:
1.Theabovetestingisreservedforthoseinstanceswhenapatientcomplainsofadeficitinhearing.Thus,on
thebasisofhistory,thereshouldbeacomplaintofhearingdeclineinoneorbothears.
2.Inthesettingofaconductivehearingloss(e.g.waxintheexternalcanal),theWebbertestwilllateralize
(i.e.soundwillbeheardbetter)intheearthathasthesubjectivedeclineinhearing.Thisisbecausewhen
thereisaproblemwithconduction,competingsoundsfromtheoutsidecannotreachCN8viatheexternal
canal.Thus,soundgeneratedbythevibratingtuningforkandtravelingtoCN8bymeansofbony
conductionisbetterheardasithasnooutside"competition."Youcantransientlycreateaconductive
hearinglossbyputtingthetipofyourindexfingerintheexternalcanalofoneear.Ifyoudothiswhile
performingtheWebbertest,thesoundwillbeheardonthatside.
3.Inthesettingofasensorineuralhearingloss(e.g.atumorofCN8),theWebbertestwilllateralizetothe
earwhichdoesnothavethesubjectivedeclineinhearing.ThisisbecauseCN8isthefinalpathway
throughwhichsoundiscarriedtothebrain.Thus,eventhoughthebonesoftheskullwillsuccessfully
transmitthesoundtoCN8,itcannotthenbecarriedtothebrainduetotheunderlyingnervedysfunction.
4.Inthesettingofconductivehearingloss,boneconduction(BC)willbebetterthenairconduction(AC)
whenassessedbytheRinneTest.Ifthereisablockageinthepassageway(e.g.wax)thatcarriessound
fromtheoutsidetoCN8,thensoundwillbebetterheardwhenittravelsviathebonesoftheskull.Thus,
thepatientwillnoteBCtobebetterthenorequaltoACintheearwiththesubjectivedeclineinhearing.
5.Inthesettingofasensorineuralhearingloss,airconductionwillstillbebetterthenboneconduction(i.e.
thenormalpatternwillberetained).ThisisbecausetheproblemisatthelevelofCN8.Thus,regardless
ofthemeans(boneorair)bywhichtheimpulsegetstoCN8,therewillstillbeamarkedhearing
decrementintheaffectedear.AsACisnormallybetterthenBC,thiswillstillbethecase.
Summary:
https://meded.ucsd.edu/clinicalmed/neuro2.htm
15/40
9/12/2016
APracticalGuidetoClinicalMedicine
Identifyingconductivevsensorineuralhearingdeficitsrequireshistoricalinformationaswellastheresultsof
WebberandRinnetesting.Insummary,thisdataisinterpretedasfollows:
1.Firstdeterminebyhistoryandcrudeacuitytestingwhichearhasthehearingproblem.
2.PerformtheWebbertest.Ifthereisaconductivehearingdeficit,theWebberwilllateralizetotheaffected
ear.Ifthereisasensorineuraldeficit,theWebberwilllateralizetothenormalear.
3.PerformtheRinnetest.Ifthereisaconductivehearingdeficit,BCwillbegreaterthenorequaltoACin
theaffectedear.Ifthereisasensorineuralhearingdeficit,ACwillbegreaterthenBCintheaffectedear.
FormoreinformationaboutCN8,seethefollowinglinks:
YaleUniversityCranialNerveReviewSite
UniformServicesSchoolofMedicineCranialNerveReviewSite
CN9(Glosopharyngeal)andCN10(Vagus):Thesenervesareresponsibleforraisingthesoftpalateofthe
mouthandthegagreflex,aprotectivemechanismwhichpreventsfoodorliquidfromtravelingintothelungsAs
bothCNscontributetothesefunctions,theyaretestedtogether.
TestingElevationofthesoftpalate:
1.Askthepatienttoopentheirmouthandsay,"ahhhh,"causingthesoftpalatetoriseupward.
2.Lookattheuvula,amidlinestructurehangingdownfromthepalate.Ifthetongueobscuresyourview,
takeatonguedepressorandgentlypushitdownandoutoftheway.
3.TheUvulashouldriseupstraightandinthemidline.
NormalOropharynx
Interpretation:
IfCN9ontherightisnotfunctioning(e.g.inthesettingofastroke),theuvulawillbepulledtotheleft.The
oppositeoccursinthesettingofleftCN9dysfunction.
https://meded.ucsd.edu/clinicalmed/neuro2.htm
16/40
9/12/2016
APracticalGuidetoClinicalMedicine
LeftCN9Dysfunction:PatientstatuspoststrokeaffectingleftCN9.Uvulathereforepulledovertowardsright.
Beawarethatotherprocessescancausedeviationoftheuvula.Aperitonsilarabscess,forexample,willpushthe
uvulatowardstheopposite(i.e.normal)tonsil.
Leftperitonsillarabscess:infectionwithinlefttonsilhaspusheduvulatowardstheright.
TestingtheGagReflex:
1.Askthepatienttowidelyopentheirmouth.Ifyouareunabletoseetheposteriorpharynx(i.e.thebackof
theirthroat),gentlypushdownwithatonguedepressor.
2.Insomepatients,thetonguedepressoralonewillelicitagag.Inmostothers,additionalstimulationis
required.Takeacottontippedapplicatorandgentlybrushitagainsttheposteriorpharynxoruvula.This
shouldgenerateagaginmostpatients.
3.Asmallbutmeasurablepercentofthenormalpopulationhaseitheraminimalornonexistentgagreflex.
Presumably,theymakeuseofothermechanismstopreventaspiration.
Gagtestingisrathernoxious.Somepeopleareparticularlysensitivetoevenminimalstimulation.Assuch,I
wouldsuggestthatyouonlyperformthistestwhenthereisreasonablesuspicionthatpathologyexists.This
wouldincludetwomajorclinicalsituations:
1.Ifyoususpectthatthepatienthassufferedacutedysfunction,mostcommonlyinthesettingofastroke.
Thesepatientsmaycomplainof/benotedtocoughwhentheyswallow.Or,theymaysufferfromrecurrent
pneumonia.Bothoftheseeventsaresignsofaspirationoffoodcontentsintothepassagewaysofthe
https://meded.ucsd.edu/clinicalmed/neuro2.htm
17/40
9/12/2016
APracticalGuidetoClinicalMedicine
lungs.ThesepatientsmayalsohaveothercranialnerveabnormalitiesaslesionsaffectingCN9and10
oftenaffectCNs11and12,whichareanatomicallynearby.
2.Patient'ssufferingfromsuddendecreasedlevelofconsciousness.Inthissetting,theabsenceofagag
mightindicatethatthepatientisnolongerabletoreflexivelyprotecttheirairwayfromaspiration.Strong
considerationshouldbegiventointubatingthepatient,providingthemwithasecuremechanicalairway
untiltheirgeneralconditionimproves.
CN9isalsoresponsiblefortasteoriginatingontheposterior1/3ofthetongue.Asthisisrarelyaclinically
importantproblem,furtherdiscussionisnotincluded.
CN10alsoprovidesparasympatheticinnervationtotheheart,thoughthiscannotbeeasilytestedonphysical
examination.
FormoreinformationaboutCN9and10,seethefollowinglinks:
YaleUniversityCranialNerveReviewSite
UniformServicesSchoolofMedicineCranialNerveReviewSite
CN11(SpinalAccessory):CN11innervatesthemuscleswhichpermitshruggingoftheshoulders(Trapezius)
andturningtheheadlaterally(Sternocleidomastoid).
1.Placeyourhandsontopofeithershoulderandaskthepatienttoshrugwhileyouprovideresistance.
Dysfunctionwillcauseweakness/absenceofmovementontheaffectedside.
2.Placeyouropenlefthandagainstthepatient'srightcheekandaskthemtoturnintoyourhandwhileyou
provideresistance.Thenrepeatontheotherside.TherightSternocleidomasoidmuscle(andthusrightCN
11)causestheheadtoturntotheleft,andviceversa.
https://meded.ucsd.edu/clinicalmed/neuro2.htm
18/40
9/12/2016
APracticalGuidetoClinicalMedicine
CN12(Hypoglossal):CN12isresponsiblefortonguemovement.EachCN12innervatesonehalfofthetongue.
Testing:
1.Askthepatienttosticktheirtonguestraightoutoftheirmouth.
2.Ifthereisanysuggestionofdeviationtooneside/weakness,directthemtopushthetipoftheirtongue
intoeithercheekwhileyouprovidecounterpressurefromtheoutside.
Interpretation:
IftherightCN12isdysfunctional,thetonguewilldeviatetotheright.Thisisbecausethenormallyfunctioning
lefthalfwilldominateasitnolongerhasoppositionfromtheright.Similarly,thetonguewouldhavelimitedor
absentabilitytoresistagainstpressureappliedfromoutsidetheleftcheek.
LeftCN12Dysfunction:StrokehasresultedinLCN12Palsy.
Tonguethereforedeviatestotheleft.
FormoreinformationaboutCN12,seethefollowinglinks:
YaleUniversityCranialNerveReviewSite
UniformServicesSchoolofMedicineCranialNerveReviewSite
SensoryandMotorExaminationsABriefReviewofAnatomyandPhysiology:
SensoryTesting
https://meded.ucsd.edu/clinicalmed/neuro2.htm
MotorTesting
19/40
9/12/2016
APracticalGuidetoClinicalMedicine
Testingofmotorandsensoryfunctionrequiresabasicunderstandingofnormalanatomyandphysiology.In
brief:
1.Voluntarymovementbeginswithanimpulsegeneratedbycellbodieslocatedinthebrain.
2.Signalstravelfromthesecellsdowntheirrespectiveaxons,formingtheCortiospinal(a.k.a.Pyramidal)
tract.Atthelevelofthebrainstem,thismotorpathwaycrossesovertotheoppositesideofthebodyand
continuedownwardonthatsideofthespinalcord.Thenerveswhichcomprisethismotorpathwayare
collectivelyreferredtoasUpperMotorNeurons(UMNs).It'simportanttonotethatthereareothermotor
pathwaysthatcarryimpulsesfromthebraintotheperipheryandhelpmodulatemovement.Adiscussion
ofthesetractscanbefoundinotherNeurologyreferencetexts.
Formoreinformationaboutmotorpathways,seethefollowinglink:
UniversityofWashingtonReviewofMotorPathways
3.Ataspecificpointinthespinalcordtheaxonsynapseswitha2ndnerve,referredtoasaLowerMotor
Neuron(LMN).Thepreciselocationofthesynapsedependsuponwherethelowermotorneuronis
destinedtotravel.If,forexample,theLMNterminatesinthehand,thesynapseoccursinthecervical
spine(i.e.neckarea).However,ifit'sheadedforthefoot,thesynapseoccursinthelumbarspine(i.e.
lowerback).
4.TheUMNsarepartoftheCentralNervousSystem(CNS),whichiscomposedofneuronswhosecell
bodiesarelocatedinthebrainorspinalcord.TheLMNsarepartofthePeripheralNervousSystem
(PNS),madeupofmotorandsensoryneuronswithcellbodieslocatedoutsideofthebrainandspinal
cord.TheaxonsofthePNStraveltoandfromtheperiphery,connectingtheorgansofaction(e.g.
muscles,sensoryreceptors)withtheCNS.
5.NerveswhichcarryimpulsesawayfromtheCNSarereferredtoEfferents(i.e.motor)whilethosethat
bringsignalsbackarecalledAfferents(i.e.sensory).
6.Axonsthatexitandenterthespineatanygivenlevelgenerallyconnecttothesamedistalanatomicarea.
Thesebundlesofaxons,referredtoasspinalnerveroots,containbothafferentandefferentnerves.The
rootsexit/enterthespinalcordthroughneruoforaminainthespine,pairedopeningsthatallowfortheir
passageoutofthebonyprotectionprovidedbythevertebralcolumn.
Formoreinformationaboutspinalcordanatomy,seethefollowinglink:
ReviewofSpinalAnatomy
7.Astheefferentneuronstravelsperipherally,componentsfromdifferentrootscommingleandbranch,
followingahighlyprogrammedpattern.Ultimately,contributionsfromseveralrootsmaycombinetoform
anamedperipheralnerve,whichthenfollowsapreciseanatomicrouteonitswaytoinnervatingaspecific
muscle.TheRadialNerve,forexample,travelsaroundtheHumerus(boneoftheupperarm),contains
contributionsfromCervicalNerveRoots6,7and8andinnervatesmusclesthatextendthewristand
supinatetheforearm.
Itmayhelptothinkofanerverootasanelectricalcablecomposedofmanydifferentcoloredwires,each
wirerepresentinganaxon.Asthecablemovesawayfromthespinalcord,wiressplitoffandheadto
differentdestinations.Priortoreachingtheirtargets,theycombinewithwiresoriginatingfromother
cables.Thegroupofwiresthatultimatelyendsatatargetmusclegroupmaythereforehavecontributions
fromseveraldifferentroots.
Formoreinformationaboutradialnerveanatomyandfunction,seebelow.
8.Afferentscarryimpulsesintheoppositedirectionofthemotornerves.Thatis,theybringinformation
fromtheperipherytothespinalcordandbrain.
9.Sensorynervesbeginintheperiphery,receivinginputfromspecializedreceptororgans.Theaxonsthen
moveproximally,joininginaprecisefashionwithotheraxonstoformtheafferentcomponentofanamed
https://meded.ucsd.edu/clinicalmed/neuro2.htm
20/40
9/12/2016
APracticalGuidetoClinicalMedicine
peripheralnerve.TheRadialNerve,forexample,notonlyhasamotorfunction(describedpreviously)but
alsocarriessensoryinformationfromdiscretepartsofthehandandforearm.
10.Asthesensoryneuronsapproachthespinalcord,theyjoinspecificspinalnerveroots.Eachrootcarries
sensoryinformationfromadiscreteareaofthebody.Theareaofskininnervatedbyaparticularnerve
rootisreferredtoasadermatome.Dermatomemapsdescribethepreciseareasofthebodyinnervatedby
eachnerveroot.Thesedistributionsaremoreorlessthesameforallpeople,whichisclinicallyimportant.
Inthesettingofnerverootdysfunction,thespecificareasuppliedbythatrootwillbeaffected.Thiscanbe
mappedoutduringacarefulexam(seebelow),identifyingwhichroot(s)isdysfunctional.
Toviewadermatomalmap,seethefollowinglink:
DermatomeMapUniversityofScranton
11.Sensoryinputtravelsupthroughthespinalcordalongspecificpaths,withthepreciseroutedefinedbythe
typeofsensationbeingtransmitted.Nervescarryingpainimpulses,forexample,crosstotheoppositeside
ofthespinalcordsoonafterentering,andtraveluptothebrainonthatsideofthecord.Vibratory
sensations,ontheotherhand,enterthecordandtravelupthesameside,crossingoveronlywhenthey
reachthebrainstem(seefollowingsectionsfordetaileddescriptions).
Formoreinformationaboutsensorypathways,seethefollowinglink:
UniversityofWashingtonReviewofSensoryPathways
12.Ultimately,thesensorynervesterminateinthebrain,wheretheimpulsesareintegratedandperception
occurs.
Understandingtheaboveneruoanatomicrelationshipsandpatternsofinnervationhasimportantclinical
implicationswhentryingtodeterminetheprecisesiteofneurologicaldysfunction.Injuryatthespinalnerveroot
level,forexample,willproduceacharacteristiclossofsensoryandmotorfunction.Thiswilldifferfromthat
causedbyaproblemattheleveloftheperipheralnerve.Anapproachtolocalizinglesionsonthebasisofmotor
andsensoryfindingsisdescribedinthesectionswhichfollow.Realizethatthereisafairamountofinter
individualvariationwithregardstothespecificsofinnervation.Also,recognizethatoftenonlypartsofnerves
maybecomedysfunctional,leadingtopartialmotororsensorydeficits.Assuch,thepatternsoflossarerarelyas
"pure"asmightbesuggestedbytheprecisedescriptionsofnervesandtheirinnervations.
SensoryTesting
SensorytestingofthefaceisdiscussedinthesectiononCranialNerves.Testingoftheextremitiesfocuseson
thetwomainafferentpathways:SpinothalamicsandDorsalColumns.
1.Spinothalamics:Thesenervesdetectpain,temperatureandcrudetouch.Theytravelfromtheperiphery,
enterthespinalcordandthencrosstotheothersideofthecordwithinoneortwovertebrallevelsoftheir
entrypointTheythencontinueupthatsidetothebrain,terminatinginthecerebralhemisphereonthe
oppositesideofthebodyfromwheretheybegan.
2.DorsalColumns:Thesenervesdetectposition(a.k.a.proprioception),vibratorysensationandlighttouch.
Theytravelfromtheperiphery,enteringthespinalcordandthenmovinguptothebaseofthebrainonthe
samesideofthecordaswheretheystarted.Uponreachingthebrainstemtheycrosstotheoppositeside,
terminatinginthecerebralhemisphereontheoppositesideofthebodyfromwheretheybegan.
Ascreeningevaluationofthesepathwayscanbeperformedasfollows:
Spinothalamics
https://meded.ucsd.edu/clinicalmed/neuro2.htm
21/40
9/12/2016
APracticalGuidetoClinicalMedicine
1.Thepatient'sabilitytoperceivethetouchofasharpobjectisusedtoassessthepainpathwayofthe
Spinothalamics.Todothis,breakaQtiportonguedepressorinhalf,suchthatyoucreateasharp,pointy
end.Alternatively,youcanuseadisposableneedleorthesharpandbluntendsofasafetypin.Iwould
discouragetheuseofthepointy,metalspikesthataccompanysomereflexhammers.If,forexample,you
usedthisandcausedbleeding,it'spossible(ifthetipwerenotwellcleaned)totransmitbloodborne
infectionsfromonepatienttoanother.Bettertouseadisposableimplement.
2.Askthepatienttoclosetheireyessothattheyarenotabletogetvisualclues.
3.Startatthetopofthefoot.Orientthepatientbyinformingthemthatyouaregoingtofirsttouchthemwith
thesharpimplement.Thendothesamewithanonsharpobject(e.g.thesoftendofaqtip).Thisclarifies
forthepatientwhatyouaredefiningassharpanddull.
4.Now,touchthelateralaspectofthefootwitheitherthesharpordulltool,askingthemtoreporttheir
response.Movemediallyacrossthetopofthefootcrossingmultipledermatomes,notingthepatient's
responsetoeachtouch.
5.Iftheygiveaccurateresponses,dothesameontheotherfoot.Thesametestcanberepeatedfortheupper
extremities(i.e.onthehand),thoughthiswouldonlybeofutilityifthepatientcomplainedof
numbness/impairedsensationinthatarea.
6.Spinothalamictractfunctioncanalsobeassessedbycheckingthepatient'sabilitytodetectdifferencesin
temperature.Coldandwarmcanbereproducedbyrunningatuningforkunderwaterofthattemperature,
touchingitagainsttheaffectedlimb,andaskingthepatienttocomment(patient'seyesshouldbeclosed).
DorsalColumns
Proprioception:Thisreferstothebody'sabilitytoknowwhereitisinspace.Assuch,itcontributestobalance.
SimilartotheSpinothalamictracts,disorderswhichaffectthissystemtendtofirstoccuratthemostdistal
aspectsofthebody.Thus,proprioceptionischeckedfirstinthefeetandthen,ifabnormal,moreproximally(e.g.
thehands).
Technique:
1.Askthepatienttoclosetheireyessothattheydonotreceiveanyvisualcues.
2.Withonehand,graspeithersideofgreattoeattheinterphalangeal(IP)joint.Placeyourotherhandonthe
lateralandmedialaspectsofthegreattoedistaltotheIP.
3.Orientpatienttoupanddownasfollows:
Flexthetoe(pullitupwards)whiletellingpatientwhatyou'redoing.
Extendtoe(pullitdownwards)whileinformingthemofwhichdirectionyou'removingit.
https://meded.ucsd.edu/clinicalmed/neuro2.htm
22/40
9/12/2016
APracticalGuidetoClinicalMedicine
TestingProprioception
4.Alternatelydeflectthetoeupordownwithouttellingthepatientinwhichdirectionyouaremovingit.
Theyshouldbeabletocorrectlyidentifythemovementanddirection.
5.Bothgreattoesshouldbecheckedinthesamefashion.Ifnormal,nofurthertestingneedbedoneinthe
screeningexam.
6.Ifthepatientisunabletocorrectlyidentifythemovement/direction,movemoreproximally(e.g.tothe
anklejoint)andrepeat(e.g.testwhethertheycandeterminewhetherthefootismovedupordownatthe
ankle).
Similartestingcanbedoneonthefingers.Thisisusuallyreservedforthosesettingswhenpatientshavedistal
findingsand/orsymptomsintheupperextremities.
VibratorySensation:Vibratorysensationtravelstothebrainviathedorsalcolumns.Thus,thefindingsgenerated
fromtestingthissystemshouldcorroboratethoseofproprioception(seeabove).
Technique:
1.Startatthetoeswiththepatientseated.Youwillneeda128hztuningfork.
128Hztuningfork
2.Askthepatienttoclosetheireyessothattheydonotreceiveanyvisualcues.
3.Graspthetuningforkbythestemandstriketheforkedendsagainstthefloor,causingittovibrate.
https://meded.ucsd.edu/clinicalmed/neuro2.htm
23/40
9/12/2016
APracticalGuidetoClinicalMedicine
4.Placethestemontopoftheinterphalangealjointofthegreattoe.Putafewfingersofyourotherhandon
thebottomsideofthisjoint.
Testingvibratorysensation
5.Askthepatientiftheycanfeelthevibration.Youshouldbeabletofeelthesamesensationwithyour
fingersonthebottomsideofthejoint.
6.Thepatientshouldbeabletodeterminewhenthevibrationstops,whichwillcorrelatewithwhenyouare
nolongerabletofeelittransmittedthroughthejoint.Itsometimestakesawhilebeforetheforkstops
vibrating.Ifyouwanttomovethingsalong,rubtheindexfingerofthehandholdingtheforkalongthe
tines,rapidlydampeningthevibration.
Repeattestingontheotherfoot.
Additional/SpecialTestingforDorsalColumnDysfunction
TestingTwoPointDiscrimination:Patientsshouldnormallybeabletodistinguishsimultaneoustouchwith2
objectswhichareseparatedbyatleast5mm.ThesestimuliarecarriedviatheDorsalColumns.Whilenot
checkedroutinely,itisusefultestifadiscreteperipheralneruropathyissuspected(e.g.injurytotheradial
nerve).
Technique:
1.Testingcanbedonewithapaperclip,openedsuchthattheendsare5mmapart.
2.Thepatientshouldbeabletocorrectlyidentifywhetheryouaretouchingthemwithoneorbothends
simultaneously,alongtheentiredistributionofthespecificnervewhichisbeingassessed.
SpecialTestingforEarlyDiabeticNeuropathy:Acarefulfootexaminationshouldbeperformedonall
patientswithsymptomssuggestiveofsensoryneuropathyoratparticularriskforthisdisorder(e.g.anyonewith
Diabetes).Lossofsensationinthisareacanbeparticularlyproblematicasthefeetareadifficultareaforthe
patienttoevaluateontheirown.Smallwoundscanbecomelargeandinfected,unbeknownsttotheinsensate
patient.Sensorytestingasdescribedabovecandetectthistypeofproblem.Disposablemonofilaments(known
astheSemmesWeinsteinAethesiometer)arespeciallydesignedforascreeningevaluation.Thesesmallnylon
fibersaredesignedsuchthatthenormalpatientshouldbeabletofeeltheendswhentheyaregentlypressed
againstthesolesoftheirfeet.
https://meded.ucsd.edu/clinicalmed/neuro2.htm
24/40
9/12/2016
APracticalGuidetoClinicalMedicine
Monofiliment
Technique:
1.Havethepatientclosetheireyessothattheydonotreceiveanyvisualcues.
2.Touchthemonofilamentto57areasonthebottomofthepatient'sfoot.Picklocationssothatallofthe
majorareasofthesoleareassessed.Avoidcalluses,whicharerelativelyinsensate.
3.Thepatientshouldbeabletodetectthefilamentwhenthetipislightlyappliedtotheskin.
Monofilimenttesting:Patientswithnormalsensationshouldbeabletodetectthemonofilimentwhenit
islightlyapplied(pictureonleft).Iftheforcerequiredtoprovokeasensoryresponseisstrongenoughto
bendthemonofiliment
(pictureonright),thensensationisimpaired.
Interpretation:Iftheexaminerhastosupplyenoughpressuresuchthatthefilamentbendspriortothepatient
beingabletodetectit,theylikelysufferfromsensoryneuropathy.Testingshouldbedoneinmultiplespotsto
https://meded.ucsd.edu/clinicalmed/neuro2.htm
25/40
9/12/2016
APracticalGuidetoClinicalMedicine
verifytheresults.Patient'swithdistalsensoryneuropathyshouldcarefullyexaminetheirfeetandweargood
fittingshoestoassurethatskinbreakdownandinfectionsdon'tdevelop.Effortsshouldalsobemadetoclosely
controltheirdiabetessothattheneuropathydoesnotprogress.
NeuropathicUlcer:Largeulcerhasdevelopedinthispatientwithseverediabeticneuropathy.
InterpretingResultsofSensoryTesting
PatternsofImpairmentfortheSpinothalamicTracts:
1.Patientsshouldbeabletocorrectlydistinguishsharpsensation,indicatingnormalfunctionofthe
spinothalamicpathway.
2.Mappingoutregionsofimpairedsensation:Theexaminationdescribedaboveisascreeningevaluation
forevidenceofsensoryloss.Thisisperfectlyadequateinmostclinicalsettings.Occasionally,thehistory
orscreeningexaminationwillsuggestadiscreteanatomicregionthathassensoryimpairment.Whenthis
occurs,itisimportanttotryandmapouttheterritoryinvolved,usingcarefulpintestingtodefinethe
medial/lateralandproximal/distalboundariesoftheaffectedregion.Youmayevenmakepenmarkson
theskintoclearlyidentifywherethechangesoccur.Asmostclinicianshavenotmemorizedthe
distributionsofallperipheralnervesorspinalnerveroots,youcansimultaneouslyconsultareference
booktoseeifthemappedterritorymatchesaspecificnervedistribution.Thistypeofmappingis
somewhattediousandshouldonlybedoneinappropriatesituations.
3.DiffuseDistalSensoryLoss:Anumberofchronicsystemicdiseasesaffectnervefunction.Themost
commonlyoccurringofthese,atleastinWesterncountries,isDiabetes.Whencontrolhasbeenpoorover
manyyears,thesensorynervesbecomedysfunctional.Thisfirstaffectsthemostdistalaspectsofthe
nervesandthenmovesproximally.Thus,thefeetarethefirstareatobeaffected.Asitisasystemic
disease,itoccurssimultaneouslyinbothlimbs.Examrevealslossofabilitytodetectthesharpstimulus
acrosstheentirefoot.Thus,thesensorylossdoesnotfollowadermatomal(i.e.spinalnerveroot)or
peripheralnervedistribution.Astheexaminertestsmoreproximally,he/shewillultimatelyreachapoint
wheresensationisagainnormal.Themoreadvancedthedisease,thehigherupthelegthiswilloccur.
Handscanbeaffected,thoughmuchlesscommonlythenfeetasthenervestravelingtothelegsarelonger
andthusatmuchgreaterrisk.ThispatternoflossisreferredtoasaStockingorGlovedistribution
impairment,astheareainvolvedcoversanentiredistalregion,muchasasockorglovewouldcovera
footorhand.Suchdeficitsmaybeassociatedwithneuropathicpain,acontinuousburningsensation
affectingthedistalextremity.
https://meded.ucsd.edu/clinicalmed/neuro2.htm
26/40
9/12/2016
APracticalGuidetoClinicalMedicine
4.PeripheralNerveDistribution:Aspecificperipheralnervecanbecomedysfunctional.Thismight,for
example,occurastheresultoftraumaorinfarction(anothercomplicationofdiabetes).Inthissetting,
therewillbeapatternofsensoryimpairmentthatfollowsthedistributionofthenerve.Radialnervepalsy,
forexample,canoccurifanintoxicatedpersonfallsasleepinapositionthatputspressureonthenerveas
ittravelsaroundtheHumerus(boneoftheupperarm).Intoxicationinducedlossofconsciousnessthen
preventsthepatientfromreflexivelychangingposition,thenormalmeansbywhichwepreventnerves
frombeingexposedtoconstantdirectpressure.Theresultantsensorylosswouldinvolvethebackofthe
handandforearm.Motorfunctionwouldalsobeaffected(seeundermotorexam).Pinningdownthe
culpritnerverequiresknowledgeofnerveanatomyandinnervation.Onapracticallevel,mostclinicians
don'tcommitthistomemory.Rather,theygatherahistorysuggestiveofadiscretenervedeficit,verifythe
territoryoflossonexam,andthenlookitupinareferencebook.
Formoreinformationaboutperipheralnerveinjuries,seethefollowinglink:
Peripheralnervesandtheirterritoriesofinnervation
5.NerveRootImpairment:Anerveroot(orroots)canbedamagedasitleavesthecord.Thiswillresultina
sensorydeficitalongitsspecificdistribution,whichcaninturnbeidentifiedonexamination.TheS1
nerveroot,forexample,canbecompressedbyherniateddiscmaterialinthelumbarspine.Thiswould
causesensorylossalongthelateralaspectofthelowerlegandthebottomofthefoot.Onlythelegonthe
affectedsidewouldhavethisdeficit.Asmentionedunderperipheralnervedysfunction,mostcliniciansdo
notmemorizethedermatomesrelatedtoeachnerveroot.Rather,theygatherahistorysuggestiveofa
discretenervedeficit,verifyadermatomaldistributionoflossonexam,andthenlookitupinareference
book.
Formoreinformationaboutnerverootcompression,seethefollowinglinks:
UniversityofWisconsin,Anatomyandpathophysiologyofnerverootcompression
ImageofHerniatedDisk
6.TheSpinothalamicsarealsoresponsiblefortemperaturediscrimination.Forpracticalreasons(i.e.it's
oftenhardtofindtesttubes,fillthemwiththerequisitetemperaturewater,etc)thisisomittedinthe
screeningexam.Theinformationfromsharpstimulustestingasdescribedaboveshouldsuffice.
Temperaturediscriminationcouldbeassessedasameansofverifyinganyabnormalitydetectedon
sharp/dulltesting.
7.Testingofthesacralnerveroots,servingtheanusandrectum,isimportantifpatientscomplainof
incontinence,inabilitytodefecate/urinate,orthereisotherwisereasontosuspectthattheserootsmaybe
compromised.InthesettingofCaudaEquinasyndrome,forexample,multiplesacralandlumbarroots
becomecompressedbilaterally(e.g.byposteriorlyherniateddiscmaterialoratumor).Whenthisoccurs,
thepatientisunabletourinate,asthelowermotorneuronscarriedinthesesacralnerverootsnolonger
function.Thusthereisnowaytosendanimpulsetothebladderinstructingittocontract.Norwilltheybe
awarethattherebladdersarefull.Therewillalsobelossofanalspinctertone,whichcanbeappreciated
onrectalexam.Abilitytodetectpinpricksintheperinealarea(a.k.a.saddledistribution)isalso
diminished.
Formoreinformationaboutperipheralnervesandtheirterritoriesofinnervation,seethefollowinglink:
Peripheralnervesandtheirterritoriesofinnervation
PatternsofImpairmentforDorsalColumnDysfunction:
Proprioception:
https://meded.ucsd.edu/clinicalmed/neuro2.htm
27/40
9/12/2016
APracticalGuidetoClinicalMedicine
Patientsshouldbeabletocorrectlyidentifythemotionanddirectionofthetoe.InthesettingofDorsalColumn
dysfunction(acommoncomplicationofdiabetes,forexample),distaltestingwillbeabnormal.Thisissimilarto
thepatternofinjurywhichaffectstheSpinothalamictractsdescribedabove.
VibratorySensation:
1.Patientsshouldbeabletodetecttheinitialvibrationandaccuratelydeterminewhenithasstopped.
2.Asdescribedundertestingofproprioception,dorsalcolumndysfunctiontendstofirstaffectthemost
distalaspectsofthesystem.Whenthisoccurs,thepatientiseitherunabletodetectthevibrationorthey
perceivethatthesensationextinguishestooearly(i.e.theystopfeelingiteventhoughyoucanstill
appreciatethesensationwithyourfingersontheundersideofthejoint).
3.Thefindingsonvibratorytestingshouldparallelthoseobtainedwhenassessingproprioception,asboth
sensationstravelviathesamepathway.
MotorTesting
Themuscleistheunitofactionthatcausesmovement.Normalmotorfunctiondependsonintactupperand
lowermotorneurons,sensorypathwaysandinputfromanumberofotherneurologicalsystems.Disordersof
movementcanbecausedbyproblemsatanypointwithinthisinterconnectedsystem.
MuscleBulkandAppearance:
Thisassessmentissomewhatsubjectiveandquitedependentontheage,sexandtheactivity/fitnesslevelofthe
individual.Afrailelderlyperson,forexample,willhavelessmusclebulkthena25yearoldbodybuilder.With
experience,youwillgetasenseofthenormalrangeforgivenagegroups,factoringintheirparticularactivity
levelsandoverallstatesofhealth.
Thingstolookfor:
1.Usingyoureyesandhands,carefullyexaminethemajormusclegroupsoftheupperandlower
extremities.Firstyouneedtofullyexposethemusclesofbothextremities(forcomparison)thatyou're
examining.Palpationofthemuscleswillgiveyouasenseofunderlyingmass.Thelargestandmost
powerfulgroupsarethoseofthequadricepsandhamstringsoftheupperleg(i.e.frontandbackofthe
thighs).
2.Musclegroupsshouldappearsymmetricallydevelopedwhencomparedwiththeircounterpartsonthe
othersideofthebody.Theyshouldalsobeappropriatelydeveloped,aftermakingallowancesforthe
patient'sage,sex,andactivitylevel.
https://meded.ucsd.edu/clinicalmed/neuro2.htm
28/40
9/12/2016
APracticalGuidetoClinicalMedicine
MuscleAsymmetry
Whilebothlegshavewelldevelopedmusculature,thelefthasgreaterbulk.
Thereshouldbenomusclemovementwhenthelimbisatrest.Raredisorders(e.g.AmyotrophicLateral
Sclerosis)resultindeathofthelowermotorneuronandsubsequentdenervationofthemuscle.This
causestwitchingofthefibersknownasfasciculations,whichcanbeseenongrossinspectionofaffected
muscles.ALSisaccompaniedbyotherfindingsandsymptoms,inparticular,relentlesslyprogressive
weakness.MoreonALShttp://www.ninds.nih.gov/disorders/amyotrophiclateralsclerosis/ALS.htm
Anumberofmorecommon(andrelativelybenign)conditionscanalsocausefasciulations,including:post
exercise,meds,stimulants,andassortedmetabolicprocesses.
Toseeavideodemonstratingfeaturesoffasciculations,clickonthe
movieicon.
3.Tremorsareaspecifictypeofcontinuous,involuntarymuscleactivitythatresultsinlimbmovement.
Parkinson'sDisease(PD),forexample,cancauseaverycharacteristicrestingtremorofthehand(thehead
andotherbodypartscanalsobeaffected)thatdiminisheswhenthepatientvoluntarilymovestheaffected
limb.BenignEssentialTremor,ontheotherhand,persiststhroughoutmovementandisnotassociated
withanyotherneurologicalfindings,easilydistinguishingitfromPD.
Toseeavideodemonstratingfeaturesofbenignessentialtremor,click
onthemovieicon.
ToseeavideodemonstratingfeaturesofParkinson'sDisease,clickon
themovieicon.
FormoreinformationaboutParkinson'sDisease,seethefollowinglink:
NIHSponsoredSiteAboutParkinson'sDisease
4.Themajormusclegroupstobepalpatedinclude:biceps,triceps,deltoids,quadricepsandhamstrings.
Palpationshouldnotelicitpain.Interestingly,myositis(arareconditioncharacterizedbyidiopathic
https://meded.ucsd.edu/clinicalmed/neuro2.htm
29/40
9/12/2016
APracticalGuidetoClinicalMedicine
muscleinflammation)causesthepatienttoexperienceweaknessbutnotpain.
5.Ifthereisasymmetry,noteifitfollowsaparticularpattern.Rememberthatsomeallowancemustbemade
forhandedness(i.e.rightvlefthanddominance).Doestheasymmetryfollowaparticularnerve
distribution,suggestingaperipheralmotorneuroninjury?Forexample,muscleswhichlosetheirLMN
inervationbecomeveryatrophic.Isthebulkintheupperandlowerextremitiessimilar?Spinalcord
transectionattheThoraciclevelwillcauseupperextremitymusclebulktobenormalorevenincreased
duetoincreaseddependenceonarmsforactivity,mobility,etc.However,themusclesofthelower
extremitywillatrophyduetolossofinnervationandsubsequentdisuse.Isthereanotherprocess
(suggestedbyhistoryorotheraspectsoftheexam)thathasresultedinlimitedmovementofaparticular
limb?Forexample,abrokenlegthathasrecentlybeenliberatedfromacastwillappearmarkedly
atrophic.
DiffuseMuscleWasting:Notelossmusclebulkinlefthandduetoperipheraldenervation.
Inparticular,compareleftandrightthenareminences.
Tone:Whenamusclegroupisrelaxed,theexaminershouldbeabletoeasilymanipulatethejointthroughits
normalrangeofmotion.Thismovementshouldfeelfluid.Anumberofdiseasestatesmayalterthissensation.
Forthescreeningexamination,itisreasonabletolimitthisassessmenttoonlythemajorjoints,including:wrist,
elbow,shoulder,hipsandknees.
Technique:
1.Askthepatienttorelaxthejointthatistobetested.
2.Carefullymovethelimbthroughitsnormalrangeofmotion,beingcarefulnottomaneuveritinanyway
thatisuncomfortableorgeneratespain.
3.Beawarethatmanypatients,particularlytheelderly,oftenhaveothermedicalconditionsthatlimitjoint
movement.Degenerativejointdiseaseoftheknee,forexample,mightcauselimitedrangeofmotion,
thoughtoneshouldstillbenormal.Ifthepatienthasrecentlyinjuredtheareaorareinpain,donot
performthisaspectoftheexam.
Thingstolookfor:
1.Normalmusclegeneratessomeresistancetomovementwhenalimbismovedpassivelybyanexaminer.
Afterperformingthisexamonanumberofpatients,you'lldevelopanappreciationfortherangeof
normaltone.
2.Iftheexaminermovesthejoint(patientrelaxed)andthereisincreasedresistance,thisisreferredtoas
increasedtone,whichcanbefurthercharacterizedasrigidorspastic.
a.Spasticity:Toneincreasesiftheexaminermovesthejointmorequickly(i.e.thehypertonicityis
affectedbytherateofmovementofthejoint).Thisisthetypicalfindingwithanuppermotor
https://meded.ucsd.edu/clinicalmed/neuro2.htm
30/40
9/12/2016
APracticalGuidetoClinicalMedicine
neuronlesion(e.g.strokeorspinalcordinjury).
b.Rigidity:Toneremainsincreasedregardlessofhowquicklythejointismoved.Oneexampleofthis
isParkinson'sdisease,wherelimbmovementgeneratesaratchetlikesensationknownascog
wheeling.
3.Flaccidnessisthecompleteabsenceoftone.Thisoccurswhenthelowermotorneuroniscutofffromthe
musclesthatitnormallyinnervates.
Strength:Aswithmusclebulk(describedabove),strengthtestingmusttakeintoaccounttheage,sexandfitness
levelofthepatient.Forexample,afrail,elderly,bedboundpatientmayhavemuscleweaknessduetosevere
deconditioningandnottointrinsicneurologicaldisease.Interpretationmustalsoconsidertheexpectedstrength
ofthemusclegroupbeingtested.Thequadricepsgroup,forexample,shouldbemuchmorepowerfulthenthe
Biceps.
Thereisa0to5ratingscaleformusclestrength:
0/5
1/5
2/5
3/5
4/5
5/5
Nomovement
Barestflickerofmovementofthemuscle,thoughnotenoughtomovethe
structuretowhichit'sattached.
Voluntarymovementwhichisnotsufficienttoovercometheforceof
gravity.Forexample,thepatientwouldbeabletoslidetheirhandacrossa
tablebutnotliftitfromthesurface.
Voluntarymovementcapableofovercominggravity,butnotanyapplied
resistance.Forexample,thepatientcouldraisetheirhandoffatable,but
notifanyadditionalresistancewereapplied.
Voluntarymovementcapableofovercoming"some"resistance
Normalstrength
'+'and''canbeaddedtoallowformorenuancedscoringof4/5strength(e.g.,4+or4butnot5,3+or3,etc.)
Thus,apatientwhocanovercome"moderatebutnotfullresistance"mightbegraded4+.Thisisquite
subjective,withafairamountofvariabilityamongstclinicians.Ultimately,it'smostimportantthatyoudevelop
yourownsenseofwhatthesegradationsmean,allowingforinternalconsistencyandinterpretabilityofserial
measurements.
SpecificsofStrengthTestingMajorMuscleGroups:Inthescreeningexamination,itisreasonabletocheck
onlythemajormuscles/musclegroups.Moredetailedtestingcanbeperformedinthesettingof
discrete/unexplainedweakness.Thenamesofthemajormuscles/musclegroupsalongwiththespinalrootsand
peripheralnervesthatprovidetheirinnervationareprovidedbelow.Nerverootsprovidingthegreatest
contributionareprintedinbold.Moreextensivedescriptionsofindividualmusclesandtheirfunctions,along
withtheirpreciseinnervationscanbefoundinaNeurologyreferencetext.
1.Intrinsicmusclesofthehand(C8,T1):Askthepatienttospreadtheirfingersapartagainstresistance
(abduction).Thensqueezethemtogether,withyourfingersplacedinbetweeneachoftheirdigits
(adduction).Testeachhandseparately.Themuscleswhichcontroladductionandabductionofthefingers
arecalledtheInterossei,innervatedbytheUlnarNerve.
https://meded.ucsd.edu/clinicalmed/neuro2.htm
31/40
9/12/2016
APracticalGuidetoClinicalMedicine
Formoreinformationaboutfingerabductorsandadductors,seethefollowinglinks:
UniversityofWashington,Anatomyoffingerabductorsandadductors
2.Flexorsofthefingers(C7,8,T1):Askthepatienttomakeafist,squeezingtheirhandaroundtwoofyour
fingers.Ifthegripisnormal,youwillnotbeabletopullyourfingersout.Testeachhandseparately.The
FlexorDigitorumProfunduscontrolsfingerflexionandisinnervatedbytheMedian(radial1/2)andUlnar
(medial1/2)Nerves.
Formoreinformationaboutfingerflexors,seethefollowinglinks:
UniversityofWashington,Anatomyoffingerflexors1
UniversityofWashington,Anatomyoffingerflexors2
3.Wristflexion(C7,8,T1):Havethepatienttrytoflextheirwristasyouprovideresistance.Testeach
handseparately.ThemusclegroupswhichcontrolflexionareinnervatedbytheMedianandUlnarNerves.
https://meded.ucsd.edu/clinicalmed/neuro2.htm
32/40
9/12/2016
APracticalGuidetoClinicalMedicine
Formoreinformationaboutwristflexors,seethefollowinglinks:
UniversityofWashington,Anatomyofwristflexors1
UniversityofWashington,Anatomyofwristflexors2
4.Wristextension(C6,7,8):Havethepatienttrytoextendtheirwristasyouprovideresistance.Testeach
handseparately.TheExtensorRadialismusclescontrolextensionandareinnervatedbytheRadialNerve.
ClinicalCorrelate:Damagetotheradialnerveresultsinwristdrop(lossofabilitytoextendthehandat
thewrist).Thiscanoccurviaanyoneofanumberofmechanisms.Forexample,thenervecanbe
compressedagainstthehumerusforaprolongedperiodoftimewhenanintoxicatedpersonloses
consciousnesswiththeinsideaspectoftheupperarmrestingagainstasolidobject(knownasa"Saturday
NightPalsy").
Formoreinformationaboutwristextensors,seethefollowinglinks:
UniversityofWashington,Anatomyofwristextensors1
UniversityofWashington,Anatomyofwristextensors2
5.ElbowFlexion(C5,6):Themainflexor(andsupinator)oftheforearmistheBrachialisMuscle(along
withtheBicepsMuscle).Havethepatientbendtheirelbowtoninetydegreeswhilekeepingtheirpalm
directedupwards.Thendirectthemtoflextheirforearmwhileyouprovideresistance.Testeacharm
separately.ThesemusclesareinnervatedbytheMusculocutaneousNerve.
Formoreinformationaboutelbowflexors,seethefollowinglinks:
UniversityofWashington,Anatomyofelbowflexors1
UniversityofWashington,Anatomyofelbowflexors2
https://meded.ucsd.edu/clinicalmed/neuro2.htm
33/40
9/12/2016
APracticalGuidetoClinicalMedicine
6.ElbowExtension(C7,8):Themainextensoroftheforearmisthetricepsmuscle.Havethepatientextend
theirelbowagainstresistancewhilethearmisheldout(abductedattheshoulder)fromthebodyatninety
degrees.Testeacharmseparately.TheTricepsisinnervatedbytheRadialNerve.
Formoreinformationaboutelbowextensors,seethefollowinglink:
UniversityofWashington,Anatomyofelbowextensors
7.ShoulderAdduction(C5thruT1):ThemainmuscleofadductionisthePectoralisMajor,thoughthe
Latissiumusandotherscontributeaswell.Havethepatientflexattheelbowwhilethearmisheldout
fromthebodyatfortyfivedegrees.Thenprovideresistanceastheytrytofurtheradductattheshoulder.
Testeachshoulderseparately.
Formoreinformationaboutshoulderadductors,seethefollowinglinks:
UniversityofWashington,Anatomyofshoulderadductors1
UniversityofWashington,Anatomyofshoulderadductors2
8.ShoulderAbduction(C5,6):Thedeltoidmuscle,innervatedbytheaxillarynerve,isthemainmuscleof
abduction.Havethepatientflexattheelbowwhilethearmsisheldoutfromthebodyatfortyfive
degress.Thenprovideresistanceastheytrytofurtherabductattheshoulder.Testeachshoulder
separately.
https://meded.ucsd.edu/clinicalmed/neuro2.htm
34/40
9/12/2016
APracticalGuidetoClinicalMedicine
Formoreinformationaboutshoulderabductors,seethefollowinglink:
UniversityofWashington,Anatomyofshoulderabductors
9.HipFlexion(L2,3,4):Withthepatientseated,placeyourhandontopofonethighandinstructthe
patienttoliftthelegupfromthetable.ThemainhipflexoristheIliopsoasmuscle,innervatedbythe
femoralnerve.
Formoreinformationabouthipflexors,seethefollowinglinks:
UniversityofWashington,Anatomyofhipflexors1
UniversityofWashington,Anatomyofhipflexors2
10.HipExtension(L5,S1):Withthepatientlyingprone,directthepatienttolifttheirlegoffthetableagainst
resistance.Testeachlegseparately.Themainhipextensoristhegluteusmaximus,innervatedbyinferior
glutealnerve.
https://meded.ucsd.edu/clinicalmed/neuro2.htm
35/40
9/12/2016
APracticalGuidetoClinicalMedicine
Formoreinformationabouthipextensors,seethefollowinglink:
UniversityofWashington,Anatomyofhipextensors
11.HipAbduction(L4,5,S1):Placeyourhandsontheoutsideofeitherthighanddirectthepatientto
separatetheirlegsagainstresistance.Thismovementismediatedbyanumberofmuscles.
Formoreinformationabouthipabductors,seethefollowinglinks:
UniversityofWashington,Anatomyofhipabductors1
UniversityofWashington,Anatomyofhipabductors2
UniversityofWashington,Anatomyofhipabductors3
12.HipAdduction(L2,3,4):Placeyourhandsontheinneraspectsofthethighsandrepeatthemaneuver.A
numberofmusclesareresponsibleforadduction.Theyareinnervatedbytheobturatornerve.
Formoreinformationabouthipadductors,seethefollowinglinks:
UniversityofWashington,Anatomyofhipadductors1
UniversityofWashington,Anatomyofhipadductors2
UniversityofWashington,Anatomyofhipadductors3
UniversityofWashington,Anatomyofhipadductors4
13.KneeExtension(L2,3,4):Havetheseatedpatientsteadilypresstheirlowerextremityintoyourhand
againstresistance.Testeachlegseparately.Extensionismediatedbythequadricepsmusclegroup,which
isinnervatedbythefemoralnerve.
https://meded.ucsd.edu/clinicalmed/neuro2.htm
36/40
9/12/2016
APracticalGuidetoClinicalMedicine
Formoreinformationaboutkneeextensors,seethefollowinglinks:
UnivervsityofWashington,Anatomyofkneeextensors1
UnivervsityofWashington,Anatomyofkneeextensors2
UniversityofWashington,Anatomyofkneeextensors3
UniversityofWashington,Anatomyofkneeextensors4
14.Kneeflexion(L5S1,2):Havethepatientrestprone.Thenhavethempulltheirheelupandoffthetable
againstresistance.Eachlegistestedseparately.Flexionismediatedbythehamstringmusclegroup,via
branchesofthesciaticnerve.
Formoreinformationaboutkneeflexors,seethefollowinglinks:
UniversityofWashington,Anatomyofkneeflexors1
UniversityofWashington,Anatomyofkneeflexors2
UniversityofWashington,Anatomyofkneeflexors3
UniversityofWashington,Anatomyofkneeflexors4
UniversityofWashington,Anatomyofkneeflexors5
15.AnkleDorsiflexion(L4,5):Directthepatienttopulltheirtoesupwardswhileyouprovideresistancewith
yourhand.Eachfootistestedseparately.Themuscleswhichmediatedorsiflexionareinnervatedbythe
deepperonealnerve.ClinicalCorrelate:Theperonealnerveissusceptibletoinjuryatthepointwhereit
crossestheheadofthefibula(laterally,belowtheknee).Ifinjured,thepatientdevelops"FootDrop,"an
inabilitytodorsiflexthefoot.
https://meded.ucsd.edu/clinicalmed/neuro2.htm
37/40
9/12/2016
APracticalGuidetoClinicalMedicine
Formoreinformationaboutankledorsiflexors,seethefollowinglink:
UniversityofWashington,Anatomyofankledorsiflexors
16.AnklePlantarFlexion(S1,S2).Havethepatient"steponthegas"whileprovidingresistancewithyour
hand.Testeachfootseparately.Thegastrocnemiusandsoleus,themuscleswhichmediatethismovement,
areinnervatedbyabranchofthesciaticnerve.Plantarflexionanddorsiflexioncanalsobeassessedby
askingthepatienttowalkontheirtoes(plantarflexion)andheels(dorsiflexion).
Formoreinformationaboutankleplantarflexors,seethefollowinglinks:
UniversityofWashington,Anatomyofankleplantarflexors1
UniversityofWashington,Anatomyofankleplantarflexors2
UniversityofWashington,Anatomyofankleplantarflexors3
Itisgenerallyquitehelpfultodirectlycomparerightvleftsidedstrength,astheyshouldmoreorlessbe
equivalent(takingintoaccountthehandednessofthepatient).Ifthereisweakness,trytoidentifyapattern,
whichmightprovideaclueastotheetiologyoftheobserveddecreaseinstrength.Inparticular,makenoteof
differencesbetween:
1.RightvLeft
2.Proximalmusclesvdistal
3.Upperextremitiesvlower
4.Oristheweaknessgeneralized,suggestiveofasystemicneurologicaldisorderorglobaldeconditioning
SpecialTestingforsubtleweakness:Subtleweaknesscanbehardtodetect.Payattentiontohowthepatient
walks,usesandholdstheirarmsandhandsastheyentertheroom,getupanddownfromaseatedposition,
moveontotheexaminationtable,etc.Pronatordriftisatestforslightweaknessoftheupperextremities.The
https://meded.ucsd.edu/clinicalmed/neuro2.htm
38/40
9/12/2016
APracticalGuidetoClinicalMedicine
patientshouldsitwithbotharmsextended,palmsdirectedupward.Subtleweaknessineitherarmwillcause
slightdownwarddriftandpronationofthatlimb(i.e.thearmwillrotateslightlyinwardanddown).
Commonperipheralnerves,territoriesofinnervation,andclinicalcorrelates.
CommonPeripheralNervesandTheirAnatomy
Peripheral
SensoryInnervation
Nerve
Motor
Innervation
Contributing
SpinalNerve Clinical
Roots
Atriskforcompressionat
humerus,knownas
"SaturdayNightPalsy"
Radial
Nerve
Backofthumb,index,
middle,and1/2ring
fingerbackof
forearm
Wrist
extensionand
abductionof
thumbin
palmerplane
Ulnar
Nerve
Palmaranddorsal
aspectsofpinkyand
1/2ofringfinger
Abductionof
fingers
(intrinsic
musclesof
hand)
Median
Nerve
Palmaraspectofthe
thumb,index,middle
and1/2ringfinger
palmbelowthese
fingers.
Abductionof
thumb
perpendicular C8,T1
topalm(thenar
muscles).
Compressionatcarpal
tunnelcausescarpaltunnel
syndrome
Canbecomecompressedin
obesepatients,causing
numbnessoverits
distribution
Lateral
Cutaneous
Nerveof
Thigh
Peroneal
Lateralaspectthigh
C6,7,8
RadialNervePalsyImage
RadialNervePalsyVideo
C7,8andT1
L1,2
Dorsiflexionof
foot(tibialis
Lateralleg,topoffoot
L4,5S1
anterior
muscle)
Atriskforinjurywith
elbowfracture.Canget
transientsymptomswhen
insideofelbowisstruck
("funnybone"distribution)
Canbeinjuredwith
proximalfibulafracture,
leadingtofootdrop
(inabilitytodorsiflexfoot)
FootDropvideo
Thistableprovidesinformationaboutusualpatternsofinnervations.Thereisoccasionallyinterindividual
variation.Inthesettingofperipheralnervedysfunction,thelevelofthelesionwilldeterminetheextentofthe
deficit.Thatis,proximalinsultswillcausetheentirenervedistributiontobeaffectedwhilemoredistallesions
willonlyimpactfunctionbeyondthesiteoftheinjury.
Moreoncarpaltunnelsyndrome...
Videooffindingsinadvancedcarpaltunnel
syndrome.
CarpalTunnelInducedAtrophy:Chronic,severecompressionofthemediannerve
withinthecarpaltunnelhasledtoatrophyoftheThenarmuscles(handonright).A
https://meded.ucsd.edu/clinicalmed/neuro2.htm
39/40
9/12/2016
APracticalGuidetoClinicalMedicine
normalappearingThenarEminenceis
demonstratedonleft.
Cranial
Nerves
SensoryandMotor
Examinations
ReflexTesting Coordination
Gait
Testing
MakingSenseof
NeurologicalFindings
Home|ClinicalImages|ForOurStudents|BioMedLibrary|Next
Copyright2015,TheRegentsoftheUniversityofCalifornia.
Allrightsreserved.Lastupdated10/15.
https://meded.ucsd.edu/clinicalmed/neuro2.htm
40/40
You might also like
- Clinical Skills Review: Scenarios Based on Standardized PatientsFrom EverandClinical Skills Review: Scenarios Based on Standardized PatientsRating: 4 out of 5 stars4/5 (10)
- SBAs and EMQs For Human Disease (Medicine) in Dentistry (2021)Document209 pagesSBAs and EMQs For Human Disease (Medicine) in Dentistry (2021)Mohammad Ibrahim100% (1)
- Ebook Ebook PDF Building A Medical Vocabulary With Spanish Translations 10Th Edition All Chapter PDF Docx KindleDocument47 pagesEbook Ebook PDF Building A Medical Vocabulary With Spanish Translations 10Th Edition All Chapter PDF Docx Kindledonald.ward211100% (22)
- A Practical Guide To Clinical MedicineDocument5 pagesA Practical Guide To Clinical Medicinejjj100% (3)
- Aaos2013Document114 pagesAaos2013Anonymous 43mqs5pElf100% (1)
- Respiratory Care Review: An Intense Look at Respiratory Care Through Case StudiesFrom EverandRespiratory Care Review: An Intense Look at Respiratory Care Through Case StudiesNo ratings yet
- FRCS Oral & Maxillofacial Surgery Part 2 100 Clinical CasesDocument426 pagesFRCS Oral & Maxillofacial Surgery Part 2 100 Clinical CasesHelena KalmatNo ratings yet
- Pearls of Glaucoma ManagementDocument576 pagesPearls of Glaucoma Managementrobeye100% (1)
- A Practical Guide To Clinical MedicineDocument6 pagesA Practical Guide To Clinical MedicineHo Lee SheetNo ratings yet
- Case PresentationDocument15 pagesCase PresentationmaymymayNo ratings yet
- Association Between Quality of Life and Anxiety, Depression, Physical Activity and Physical Performance in Maintenance Hemodialysis PatientsDocument10 pagesAssociation Between Quality of Life and Anxiety, Depression, Physical Activity and Physical Performance in Maintenance Hemodialysis PatientspangaribuansantaNo ratings yet
- Literature Review of Facial PalsyDocument4 pagesLiterature Review of Facial Palsyfvet7q93100% (1)
- Ebook Hesi Comprehensive Review For The Nclex PN Examination PDF Full Chapter PDFDocument67 pagesEbook Hesi Comprehensive Review For The Nclex PN Examination PDF Full Chapter PDFjoan.aronow184100% (28)
- Hesi Comprehensive Review For The Nclex PN Examination Hesi Full ChapterDocument67 pagesHesi Comprehensive Review For The Nclex PN Examination Hesi Full Chapterjosefa.mccollum806100% (13)
- Evidence-Based LaryngologyFrom EverandEvidence-Based LaryngologyDavid E. RosowNo ratings yet
- Evaluation of The Child With Global Developmental DelayDocument14 pagesEvaluation of The Child With Global Developmental DelayplaincircleNo ratings yet
- DNB Cardiology ThesisDocument5 pagesDNB Cardiology Thesisgloriayoungdesmoines100% (3)
- MedicalCheckUp - Physical Examination PDFDocument3 pagesMedicalCheckUp - Physical Examination PDFCielo Baez ArceNo ratings yet
- Hesi Comprehensive Review For The Nclex RN Examination 6E Oct 3 2019 - 0323582451 - Elsevier Hesi Full ChapterDocument67 pagesHesi Comprehensive Review For The Nclex RN Examination 6E Oct 3 2019 - 0323582451 - Elsevier Hesi Full Chaptertracy.zimmer564100% (14)
- PIIS0002939422003828Document7 pagesPIIS0002939422003828Anca Florina GaceaNo ratings yet
- Grubbs2014Document7 pagesGrubbs2014Anggia BungaNo ratings yet
- NPMCN DissertationDocument4 pagesNPMCN DissertationHelpWritingMyPaperCanada100% (1)
- Alcohol and Low Back Pain A Systematic Literature ReviewDocument4 pagesAlcohol and Low Back Pain A Systematic Literature RevieweubvhsvkgNo ratings yet
- Esotropia and ExotropiaDocument49 pagesEsotropia and ExotropiaEdoga Chima EmmanuelNo ratings yet
- Aha ThesisDocument7 pagesAha ThesisBuyingCollegePapersOnlineSingapore100% (2)
- Pathophysiology Concepts of Altered Health States Porth 8th Edition Test BankDocument36 pagesPathophysiology Concepts of Altered Health States Porth 8th Edition Test Banksetonwedded3urss0100% (43)
- Hesi Comprehensive Review For The Nclex RN Examination E Book Hesi Full ChapterDocument67 pagesHesi Comprehensive Review For The Nclex RN Examination E Book Hesi Full Chaptertracy.zimmer564100% (15)
- Exercise Physiology for the Pediatric and Congenital CardiologistFrom EverandExercise Physiology for the Pediatric and Congenital CardiologistNo ratings yet
- Edinburgh Research Explorer: Physical Activity For Cognitive and Mental Health in YouthDocument28 pagesEdinburgh Research Explorer: Physical Activity For Cognitive and Mental Health in Youthlauracastillolopez2000No ratings yet
- Ni Hms 400939Document16 pagesNi Hms 400939Gerad Cookie OrtegaNo ratings yet
- Rajiv Gandhi University Thesis Topics ProsthodonticsDocument8 pagesRajiv Gandhi University Thesis Topics ProsthodonticsPaperWritersAlbuquerque100% (2)
- Endo ManualDocument211 pagesEndo ManualAjay IyerNo ratings yet
- Thesis CardiovascularDocument4 pagesThesis Cardiovascularhoffklawokor1974100% (2)
- 26 Audh Ampun Aduh AmpunDocument3 pages26 Audh Ampun Aduh Ampundel AjjahNo ratings yet
- Original Article Oral Clefts and Academic Performance in Adolescence: The Impact of Anesthesia-Related Neurotoxicity, Timing of Surgery, and Type of Oral CleftsDocument10 pagesOriginal Article Oral Clefts and Academic Performance in Adolescence: The Impact of Anesthesia-Related Neurotoxicity, Timing of Surgery, and Type of Oral CleftsJocelineThedaNo ratings yet
- Usd Red Usd RedDocument43 pagesUsd Red Usd RedDr. Adel AlhusainiNo ratings yet
- Thesis Topics in Pediatric AnaesthesiaDocument7 pagesThesis Topics in Pediatric Anaesthesiaafknlbbnf100% (2)
- She Vell 2003Document15 pagesShe Vell 2003Ivan VeriswanNo ratings yet
- Evaluation of The Child With Global Developmental DelayDocument14 pagesEvaluation of The Child With Global Developmental DelaylauramwoodyardNo ratings yet
- Three Barriers Prevent Better Dialysis - New PrintDocument7 pagesThree Barriers Prevent Better Dialysis - New PrintVen LamasanNo ratings yet
- Litigation in Otolaryngology: Minimizing Liability and Preventing Adverse OutcomesFrom EverandLitigation in Otolaryngology: Minimizing Liability and Preventing Adverse OutcomesJean Anderson EloyNo ratings yet
- 'OET' SAMPLE READING NEW DR TANJIM OVEE 2020Document19 pages'OET' SAMPLE READING NEW DR TANJIM OVEE 2020AHMED TANJIMUL ISLAMNo ratings yet
- Dise Expert Consensus-Aao-2021Document14 pagesDise Expert Consensus-Aao-2021Alejandra Oliveros VargasNo ratings yet
- Pediatric Cardiology Thesis TopicsDocument4 pagesPediatric Cardiology Thesis Topicspzblktgld100% (2)
- Es La Actividad Física Un Potencial Factor Preventivo para La Demencia Vascular?Document11 pagesEs La Actividad Física Un Potencial Factor Preventivo para La Demencia Vascular?Gonzalo Sebastian Bravo RojasNo ratings yet
- Hen 206 13Document8 pagesHen 206 13Alneo LesagNo ratings yet
- Content ServerDocument16 pagesContent ServerNurul Afika LubisNo ratings yet
- Tbi ThesisDocument6 pagesTbi ThesisPaperWritingServicesForCollegeStudentsUK100% (2)
- Adhd Research Paper PDFDocument7 pagesAdhd Research Paper PDFgw1w9reg100% (1)
- MD Pulmonary Medicine Thesis TopicsDocument5 pagesMD Pulmonary Medicine Thesis Topicsamandareedsalem100% (2)
- Literature Review On Chronic Kidney DiseaseDocument10 pagesLiterature Review On Chronic Kidney Diseaseea4c954q100% (1)
- Compartment Syndrome PDFDocument187 pagesCompartment Syndrome PDFAmayaNo ratings yet
- Evaluation and Referral For Developmental Dysplasia of The Hip in Infants 2016Document13 pagesEvaluation and Referral For Developmental Dysplasia of The Hip in Infants 2016LUIS FRANCISCO GUERRERO MARTÍNEZNo ratings yet
- Orthodontic Evidence A Qampa Handbook 9783031244223 9783031244216 3031244222Document344 pagesOrthodontic Evidence A Qampa Handbook 9783031244223 9783031244216 3031244222mariam55abuzeidNo ratings yet
- PCOS ProgramBookDocument69 pagesPCOS ProgramBookDreamNo ratings yet
- Domain5 Lesson2 Getting A PhysicalDocument3 pagesDomain5 Lesson2 Getting A PhysicalMetztli Ximena MonteroNo ratings yet
- Filedate 823Document77 pagesFiledate 823ester.lingberg332No ratings yet
- Defining The Clinical Course of Multiple Sclerosis: The 2013 RevisionsDocument10 pagesDefining The Clinical Course of Multiple Sclerosis: The 2013 RevisionsTimaEmaNo ratings yet
- Idiopathic Short Stature Definition EpidDocument9 pagesIdiopathic Short Stature Definition Epidfrancisco perezNo ratings yet
- Hasil MRI Ditemukan Massa Kistik Pada Episentrum Serebellar Hemisfer KananDocument1 pageHasil MRI Ditemukan Massa Kistik Pada Episentrum Serebellar Hemisfer KananIustitia Septuaginta SambenNo ratings yet
- Hasil MRI Ditemukan Massa Kistik Pada Episentrum Serebellar Hemisfer KananDocument1 pageHasil MRI Ditemukan Massa Kistik Pada Episentrum Serebellar Hemisfer KananIustitia Septuaginta SambenNo ratings yet
- Chapter 257: Head Trauma: Introduction and EpidemiologyDocument35 pagesChapter 257: Head Trauma: Introduction and EpidemiologyIustitia Septuaginta SambenNo ratings yet
- Daftar Pustaka OEDocument1 pageDaftar Pustaka OEIustitia Septuaginta SambenNo ratings yet
- Komplikasi Kehamilan Awal Dan Definisi Baru Tentang KeguguranDocument2 pagesKomplikasi Kehamilan Awal Dan Definisi Baru Tentang KeguguranIustitia Septuaginta SambenNo ratings yet
- Orbita: (Malar) Bone, and Maxilla Form A Sturdy Approximately Circular Bony Aperture That IsDocument1 pageOrbita: (Malar) Bone, and Maxilla Form A Sturdy Approximately Circular Bony Aperture That IsIustitia Septuaginta SambenNo ratings yet
- Laring Faring FinalDocument32 pagesLaring Faring FinalIustitia Septuaginta SambenNo ratings yet
- Radiologic Diagnosis CVTDocument12 pagesRadiologic Diagnosis CVTIustitia Septuaginta SambenNo ratings yet
- A Practical Guide To Clinical Medicine-NeurologyDocument40 pagesA Practical Guide To Clinical Medicine-NeurologyIustitia Septuaginta SambenNo ratings yet
- Neuro Exam - Clinical NeurologyDocument38 pagesNeuro Exam - Clinical NeurologyIustitia Septuaginta SambenNo ratings yet
- Basic Radiology BrainDocument87 pagesBasic Radiology BrainIustitia Septuaginta SambenNo ratings yet
- Pulmonary SarcoidosisDocument22 pagesPulmonary SarcoidosisVeeru KuppastNo ratings yet
- A Practical Guide To Clinical Medicine-NeurologyDocument40 pagesA Practical Guide To Clinical Medicine-NeurologyIustitia Septuaginta SambenNo ratings yet
- Williams Hematology-Trombolytic For StrokeDocument6 pagesWilliams Hematology-Trombolytic For StrokeIustitia Septuaginta SambenNo ratings yet
- Stroke CtscanDocument21 pagesStroke CtscanIustitia Septuaginta SambenNo ratings yet
- Clinical Neurology StrokeDocument57 pagesClinical Neurology StrokeIustitia Septuaginta SambenNo ratings yet
- Basic Radiology BrainDocument87 pagesBasic Radiology BrainIustitia Septuaginta SambenNo ratings yet
- Diskusi Topik EdemaDocument1 pageDiskusi Topik EdemaIustitia Septuaginta SambenNo ratings yet
- A Practical Guide To Clinical Medicine-NeurologyDocument40 pagesA Practical Guide To Clinical Medicine-NeurologyIustitia Septuaginta SambenNo ratings yet
- Management of Skin MalignancyDocument5 pagesManagement of Skin MalignancyIustitia Septuaginta SambenNo ratings yet
- Edema 130706211220 Phpapp02Document9 pagesEdema 130706211220 Phpapp02Iustitia Septuaginta SambenNo ratings yet
- Intra Arterial Thrombo Lys IsDocument10 pagesIntra Arterial Thrombo Lys IsIustitia Septuaginta SambenNo ratings yet
- Mechanism of OedemaDocument9 pagesMechanism of OedemaIustitia Septuaginta SambenNo ratings yet
- Myocardial IschaemiaDocument20 pagesMyocardial IschaemiaIustitia Septuaginta SambenNo ratings yet
- Anatomi Lung and PleuraDocument14 pagesAnatomi Lung and PleuraIustitia Septuaginta SambenNo ratings yet
- Mechanism of EdemaDocument9 pagesMechanism of EdemaIustitia Septuaginta SambenNo ratings yet
- EdemaDocument9 pagesEdemaIustitia Septuaginta SambenNo ratings yet
- How Is Breast Cancer StagedDocument29 pagesHow Is Breast Cancer StagedIustitia Septuaginta SambenNo ratings yet