You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Lista de Verbos Regulares e IrregularesDocument11 pagesLista de Verbos Regulares e IrregularesHenry Valverde100% (1)
- Excercises: She Had Been Studying Had Not Be Walking Had You Been Doing Had Been Working Had Not Been EatingDocument2 pagesExcercises: She Had Been Studying Had Not Be Walking Had You Been Doing Had Been Working Had Not Been EatingJesus RiveraNo ratings yet
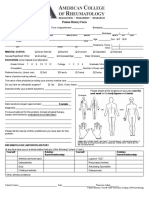
- New Patient Form PDFDocument4 pagesNew Patient Form PDFJesus RiveraNo ratings yet
- New Patient History FormDocument6 pagesNew Patient History Formعمر الرواشدة الضيغميNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Đề Thi Tủ Pte Helper 2Document52 pagesĐề Thi Tủ Pte Helper 2Văn Hữu ĐạtNo ratings yet
- 276) 2010 Cerio - Mechanism Action Clinical Benefits Colloidal Oatmeal Dermatologic PracticeDocument5 pages276) 2010 Cerio - Mechanism Action Clinical Benefits Colloidal Oatmeal Dermatologic Practicezebulon78No ratings yet
- Biphasic and Polyphasic SleepDocument6 pagesBiphasic and Polyphasic SleepalNo ratings yet
- Panangbigbig Ken Panangisurat Kadagiti Numero Manipud 0 Aginggana 100Document4 pagesPanangbigbig Ken Panangisurat Kadagiti Numero Manipud 0 Aginggana 100EVANGELINE DARRASNo ratings yet
- Evacuation Earthquake PlanDocument9 pagesEvacuation Earthquake PlanShane Giacinth AmarilaNo ratings yet
- Aspiracion Destornillador Implanto Roa-V1-Id1018Document3 pagesAspiracion Destornillador Implanto Roa-V1-Id1018CesarAmorotoNo ratings yet
- What Is RCM and RBIDocument2 pagesWhat Is RCM and RBIChihiya Fitria Nurhayati0% (1)
- Reasons For Managing Health and SafetyDocument3 pagesReasons For Managing Health and SafetybrightNo ratings yet
- Psychometric Properties of The Consensus Sleep Diary in Those With Insomnia DisorderDocument19 pagesPsychometric Properties of The Consensus Sleep Diary in Those With Insomnia DisorderMondlTNo ratings yet
- Executive SummaryDocument11 pagesExecutive Summarykhurt handrieNo ratings yet
- 491 Exam 1 KEYDocument10 pages491 Exam 1 KEYLily M Mo100% (1)
- Medical Examiner'S Confidential ReportDocument2 pagesMedical Examiner'S Confidential ReportParesh BorboruahNo ratings yet
- SMK Sinar Bintang, Segambut Kuala Lumpur Yearly Plan Science Form 3Document16 pagesSMK Sinar Bintang, Segambut Kuala Lumpur Yearly Plan Science Form 3Azie HarunNo ratings yet
- Nursing Care Plan 2 Knowledge DeficitDocument7 pagesNursing Care Plan 2 Knowledge Deficitdbryant0101100% (3)
- Human Rights (ROTC)Document6 pagesHuman Rights (ROTC)shujin_samaNo ratings yet
- Laporan IKM KSM PK FEBRUARI 2022Document28 pagesLaporan IKM KSM PK FEBRUARI 2022Nur iffahNo ratings yet
- 2019 Annual Report (Final)Document38 pages2019 Annual Report (Final)gjsdizonNo ratings yet
- Health Tourism Presentation IBMDocument65 pagesHealth Tourism Presentation IBMMd. Ashraf Hossain SarkerNo ratings yet
- From The Cocoon To The ButterflyDocument26 pagesFrom The Cocoon To The ButterflyParamita BanerjeeNo ratings yet
- BT RA 01 WeldingDocument6 pagesBT RA 01 Weldingnandha gopalNo ratings yet
- Nursepreneurs Essay by J. BacarisasDocument17 pagesNursepreneurs Essay by J. BacarisasCris GalendezNo ratings yet
- Family Reunification Plan Template FINAL 8-31-17 Incl. Appendices Pages All PortraitDocument146 pagesFamily Reunification Plan Template FINAL 8-31-17 Incl. Appendices Pages All PortraitLloyd Angelo SobredillaNo ratings yet
- Substance Use Disorders Among Youth in The Juvenile Justice SystemDocument14 pagesSubstance Use Disorders Among Youth in The Juvenile Justice SystemJames JerryNo ratings yet
- TDR Business Plan 2008-2013: Robert RidleyDocument43 pagesTDR Business Plan 2008-2013: Robert RidleySripal JainNo ratings yet
- Outpatient Dental & Clinical - Claim FormDocument1 pageOutpatient Dental & Clinical - Claim FormYiki TanNo ratings yet
- Blood Cancer Analysis by A.G.Sureshbabu ShenoyDocument4 pagesBlood Cancer Analysis by A.G.Sureshbabu Shenoysaptarishis astrologyNo ratings yet
- Holistic WellnessDocument541 pagesHolistic WellnessSeba FounderNo ratings yet
- Reflection PaperDocument27 pagesReflection PaperBon Ryan LeonardoNo ratings yet
- Nursing Skills ChecklistDocument8 pagesNursing Skills Checklistapi-353656227No ratings yet