You might also like
- Atlantis Steve JacksonDocument131 pagesAtlantis Steve Jacksonmarinboy55100% (6)
- List of Reference BooksDocument2 pagesList of Reference Booksweeda zabihNo ratings yet
- IPEC 561 SyllabusDocument6 pagesIPEC 561 SyllabusShenNo ratings yet
- Test Bank For Medical Genetics 4th Edition Lynn B JordeDocument8 pagesTest Bank For Medical Genetics 4th Edition Lynn B Jorderoytuyenbau100% (1)
- The Audio PANCE and PANRE Episode 13Document4 pagesThe Audio PANCE and PANRE Episode 13The Physician Assistant LifeNo ratings yet
- 63d0f228e52b8 Basic Geriatric Nursing 7th Edition Williams Test BankDocument108 pages63d0f228e52b8 Basic Geriatric Nursing 7th Edition Williams Test Bankerickomusiq7No ratings yet
- Diseases of The CvsDocument24 pagesDiseases of The CvsHussein Al SaediNo ratings yet
- Common Bacteria by Site of Infection: Mouth Skin/Soft Tissue Bone and JointDocument72 pagesCommon Bacteria by Site of Infection: Mouth Skin/Soft Tissue Bone and JointMuthia FadhilaNo ratings yet
- A Historical Examination of Concrete PDFDocument324 pagesA Historical Examination of Concrete PDFMa Ria Fe100% (1)
- MS Access FundamentalsDocument373 pagesMS Access Fundamentalskggan8678No ratings yet
- 2018 Fall Geriatrics SyllabusDocument41 pages2018 Fall Geriatrics SyllabusSen SioNo ratings yet
- Introduction and Overview of Community Health Nursing: Mary Ann Rosa MSN, RN, CS, GNPDocument66 pagesIntroduction and Overview of Community Health Nursing: Mary Ann Rosa MSN, RN, CS, GNPphoenix18075% (4)
- Anemia HemoliticaDocument14 pagesAnemia Hemoliticadahiana madrid quinteroNo ratings yet
- Osteotomias PediatriaDocument13 pagesOsteotomias PediatriaM Ram CrraNo ratings yet
- Perthes Disease: by Dr. Abdul Karim Postgraduate Resident Orthopedic Surgery Pgmi/Lgh. Lahore PakistanDocument68 pagesPerthes Disease: by Dr. Abdul Karim Postgraduate Resident Orthopedic Surgery Pgmi/Lgh. Lahore Pakistandrakkashmiri50% (2)
- Internal Medicine Sample Osce Examination Component Questions eDocument2 pagesInternal Medicine Sample Osce Examination Component Questions eGhada ElhassanNo ratings yet
- A. Inflammation and Repair: I. Disease Process (6 Questions)Document17 pagesA. Inflammation and Repair: I. Disease Process (6 Questions)Anonymous Sw4Pk9fNo ratings yet
- C 37Document9 pagesC 37Tammie Gore100% (3)
- D.C Circuits Class TestDocument1 pageD.C Circuits Class TestShinde JayakrishnaNo ratings yet
- Personal Fitness WorkbookDocument13 pagesPersonal Fitness WorkbookScott KramerNo ratings yet
- Test Bank For Radiographic Pathology For Technologists 7th Edition by KowalczykDocument8 pagesTest Bank For Radiographic Pathology For Technologists 7th Edition by KowalczykAudrey Snook100% (32)
- Chapter 38: Cardiovascular Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument7 pagesChapter 38: Cardiovascular Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet
- Viii. PathophysiologyDocument2 pagesViii. Pathophysiologymacedon145377No ratings yet
- BT102 - Microbiology (Solved Questions FINAL TERM (PAST PAPERS)Document33 pagesBT102 - Microbiology (Solved Questions FINAL TERM (PAST PAPERS)Awais BhuttaNo ratings yet
- C 40Document11 pagesC 40Tammie Gore100% (5)
- C 26Document9 pagesC 26Tammie GoreNo ratings yet
- Chapter 41: Alterations of Digestive Function: 1. A. C. B. D. Ans: BDocument11 pagesChapter 41: Alterations of Digestive Function: 1. A. C. B. D. Ans: BTammie GoreNo ratings yet
- C 38Document10 pagesC 38Tammie Gore100% (2)
- C 8Document11 pagesC 8Tammie Gore100% (5)
- C 17Document12 pagesC 17Tammie Gore100% (1)
- C 32Document14 pagesC 32Tammie Gore100% (8)
- C 6Document4 pagesC 6Tammie Gore100% (2)
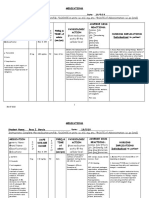
- Instructions: Complete The Medication Profile. DOSAGE in Units: I.E. ML/, MG, Etc. ROUTE of Administration: I.E. Po (Oral)Document12 pagesInstructions: Complete The Medication Profile. DOSAGE in Units: I.E. ML/, MG, Etc. ROUTE of Administration: I.E. Po (Oral)Rosa Garcia100% (1)
- C 9Document11 pagesC 9Tammie Gore100% (6)
- C 3Document12 pagesC 3Tammie Gore100% (4)
- C 24Document9 pagesC 24Tammie GoreNo ratings yet
- California Long-Term Care Programs: Recommendations To Improve Access For CaliforniansDocument329 pagesCalifornia Long-Term Care Programs: Recommendations To Improve Access For CaliforniansLeslie HendricksonNo ratings yet
- 2017 Nut116bl - Mini Case Study 3Document5 pages2017 Nut116bl - Mini Case Study 3api-347153077No ratings yet
- General Chemistry I Syllabus: Course InformationDocument4 pagesGeneral Chemistry I Syllabus: Course InformationSierra Skye MuganNo ratings yet
- Chem 124 SyllabusDocument4 pagesChem 124 SyllabuscuriousbookwormNo ratings yet
- Chem 1004 Supplement Spring 2017Document11 pagesChem 1004 Supplement Spring 2017Grant NilsonNo ratings yet
- CHM 2046L Syllabus-Fall 2014Document6 pagesCHM 2046L Syllabus-Fall 2014Amira CatoNo ratings yet
- Module 3: Pain Medications: TasksDocument9 pagesModule 3: Pain Medications: TasksSheril MarekNo ratings yet
- GastrointestinalDocument2 pagesGastrointestinalJackie Bringhurst100% (1)
- Parkinsons - Management PlanDocument3 pagesParkinsons - Management Planapi-19753815No ratings yet
- Multiple Choice Questions-Acid Base BalanceDocument6 pagesMultiple Choice Questions-Acid Base Balanceyeshi janexoNo ratings yet
- jOURNAL THEORY TTMDocument14 pagesjOURNAL THEORY TTMTrihartuty TrihartutyNo ratings yet
- Module 2: Patient/Resident Rights Minimum Number of Theory Hours: 3 Suggested Theory Hours: 5 Recommended Clinical Hours: 1 Statement of PurposeDocument23 pagesModule 2: Patient/Resident Rights Minimum Number of Theory Hours: 3 Suggested Theory Hours: 5 Recommended Clinical Hours: 1 Statement of PurposefareehaNo ratings yet
- Actual Practice On The Maagement of Care AnginaDocument96 pagesActual Practice On The Maagement of Care AnginaJaymica Laggui DacquilNo ratings yet
- Intro To Pharmacology Study GuideDocument93 pagesIntro To Pharmacology Study GuideMichelle Morgan LongstrethNo ratings yet
- PathophysExam1 Review Course HeroDocument7 pagesPathophysExam1 Review Course HeroTammie Gore100% (1)
- Anaerobic Infections in HumansFrom EverandAnaerobic Infections in HumansSydney FinegoldRating: 5 out of 5 stars5/5 (1)
- How Not to Drop Dead!: A Guide for Prevention of 201 Causes of Sudden or Rapid DeathFrom EverandHow Not to Drop Dead!: A Guide for Prevention of 201 Causes of Sudden or Rapid DeathNo ratings yet
- 2023 OB/GYN Coding Manual: Components of Correct CodingFrom Everand2023 OB/GYN Coding Manual: Components of Correct CodingNo ratings yet
- Test Bank For Body Structures and Functions 12th Edition ScottDocument9 pagesTest Bank For Body Structures and Functions 12th Edition ScottTonyRamosgbspc100% (31)
- C 20Document6 pagesC 20Tammie Gore100% (2)
- Test Bank For Human Diseases 3rd Edition NeighborsDocument13 pagesTest Bank For Human Diseases 3rd Edition Neighborsdenisedanielsbkgqyzmtr100% (25)
- PDF Test Bank For Body Structures and Functions 12Th Edition Scott Online Ebook Full ChapterDocument33 pagesPDF Test Bank For Body Structures and Functions 12Th Edition Scott Online Ebook Full Chaptermarvin.dunagan418100% (3)
- 2017 King. Etiopathogenesis of Canine Hip Dysplasia, Prevalence, and GeneticsDocument15 pages2017 King. Etiopathogenesis of Canine Hip Dysplasia, Prevalence, and GeneticsTomas CarmonaNo ratings yet
- Legg-Calve'-Perthes Disease He National Osteonecrosis FoundationDocument5 pagesLegg-Calve'-Perthes Disease He National Osteonecrosis FoundationDanica May Corpuz Comia-EnriquezNo ratings yet
- Legg-Calvé-Perthes Disease - An Overview With Recent LiteratureDocument10 pagesLegg-Calvé-Perthes Disease - An Overview With Recent LiteratureFranz BlacuttNo ratings yet
- Perthes ClasificaconesDocument3 pagesPerthes ClasificaconesABCDNo ratings yet
- Test Bank For Radiographic Pathology For Technologists 7th Edition by KowalczykDocument8 pagesTest Bank For Radiographic Pathology For Technologists 7th Edition by Kowalczykconalque0nzp9uNo ratings yet
- West Indian Medical Journal: A Case of Pathological Rib Fractures: Focal Osteolysis or Osteoporosis?Document10 pagesWest Indian Medical Journal: A Case of Pathological Rib Fractures: Focal Osteolysis or Osteoporosis?IstianahNo ratings yet
- KIM File 07 (AutoRecovered)Document70 pagesKIM File 07 (AutoRecovered)Rafey AhmedNo ratings yet
- C 48Document8 pagesC 48Tammie GoreNo ratings yet
- C 49Document8 pagesC 49Tammie GoreNo ratings yet
- C 45Document8 pagesC 45Tammie Gore100% (2)
- C 46Document10 pagesC 46Tammie GoreNo ratings yet
- PathophysExam1 Review Course HeroDocument7 pagesPathophysExam1 Review Course HeroTammie Gore100% (1)
- C 43Document10 pagesC 43Tammie Gore100% (1)
- C 47Document7 pagesC 47Tammie GoreNo ratings yet
- C 39Document8 pagesC 39Tammie Gore100% (2)
- C 44Document12 pagesC 44Tammie GoreNo ratings yet
- C 36Document9 pagesC 36Tammie Gore100% (2)
- C 34Document10 pagesC 34Tammie Gore100% (1)
- C 33Document8 pagesC 33Tammie Gore100% (2)
- C 24Document9 pagesC 24Tammie GoreNo ratings yet
- C 32Document14 pagesC 32Tammie Gore100% (8)
- C 20Document6 pagesC 20Tammie Gore100% (2)
- C 17Document12 pagesC 17Tammie Gore100% (1)
- C 30Document10 pagesC 30Tammie Gore100% (2)
- C 25Document6 pagesC 25Tammie GoreNo ratings yet
- C 23Document9 pagesC 23Tammie Gore100% (1)
- Chapter 19: Neurobiology of Schizophrenia, Mood Disorders, and Anxiety DisordersDocument7 pagesChapter 19: Neurobiology of Schizophrenia, Mood Disorders, and Anxiety DisordersTammie GoreNo ratings yet
- C 15Document10 pagesC 15Tammie Gore100% (3)
- C 14Document5 pagesC 14Tammie Gore100% (2)
- C 16Document13 pagesC 16Tammie GoreNo ratings yet
- C 18Document10 pagesC 18Tammie Gore100% (1)
- C 13Document6 pagesC 13Tammie Gore100% (1)
- D Block ElementDocument48 pagesD Block ElementPrabhakar BandaruNo ratings yet
- DLL-Take Body MeasurementDocument5 pagesDLL-Take Body MeasurementRhea GuevarraNo ratings yet
- The Iplex R: SeriesDocument6 pagesThe Iplex R: Seriesricardo sabinoNo ratings yet
- The Sims 4 CheatsDocument15 pagesThe Sims 4 CheatsthomasNo ratings yet
- Women's Marian Devotions in A Melkite Greek Catholic Village in LebanonDocument3 pagesWomen's Marian Devotions in A Melkite Greek Catholic Village in LebanonBintang Yudha Dwi KurniaNo ratings yet
- Animal Farm Revision Booklet 2.174819122Document2 pagesAnimal Farm Revision Booklet 2.174819122손지민No ratings yet
- Cost Acctg FohDocument37 pagesCost Acctg FohRizza Christine Thereza UsbalNo ratings yet
- Articles About LinguisticsDocument14 pagesArticles About LinguisticslinhhkNo ratings yet
- Afp ( Ej: The Role of Consciousness in Second LanguageDocument16 pagesAfp ( Ej: The Role of Consciousness in Second LanguageHombreMorado GamerYTNo ratings yet
- Final Spl-Enriquez - Ra 9165Document40 pagesFinal Spl-Enriquez - Ra 9165EphraimEnriquezNo ratings yet
- While: Is Not Empty Do Current Region Current Seeds Point With Minimum Curvature inDocument3 pagesWhile: Is Not Empty Do Current Region Current Seeds Point With Minimum Curvature inSanintya SeptianaNo ratings yet
- Ihw 1Document4 pagesIhw 1smagulovaNo ratings yet
- Clone Graph - LeetCodeDocument1 pageClone Graph - LeetCodejon monroeNo ratings yet
- Comeback KidsDocument77 pagesComeback KidsAline SantosNo ratings yet
- Annotation: ThemDocument4 pagesAnnotation: ThemG SravaniNo ratings yet
- By: Deepali MandaliaDocument107 pagesBy: Deepali MandaliaDeepali MandaliaNo ratings yet
- Ej 1079521Document15 pagesEj 1079521Jhoanna Castro-CusipagNo ratings yet
- FS5 QuizDocument3 pagesFS5 QuizFidel MatosNo ratings yet
- 5s-Shakeup QP Octubre 2013 PDFDocument6 pages5s-Shakeup QP Octubre 2013 PDFjavier_navlozNo ratings yet
- Blest Be The Name of Jacob's GodDocument2 pagesBlest Be The Name of Jacob's GodDenise Castilho CocareliNo ratings yet
- X-Ray Diffraction Investigation of Alloys: R. A. Butera and D. H. WaldeckDocument5 pagesX-Ray Diffraction Investigation of Alloys: R. A. Butera and D. H. WaldeckDanielleNo ratings yet
- Question Tag SlideDocument33 pagesQuestion Tag SlidekwanphylNo ratings yet
- Group 10 Battle of SiffinDocument2 pagesGroup 10 Battle of SiffinMuhammad IbrahimNo ratings yet
- Case QuestionsDocument2 pagesCase QuestionsAustinNo ratings yet