You might also like
- Nama: Desi Indah Sari NIM: 22010117130139 Kelas: CDocument2 pagesNama: Desi Indah Sari NIM: 22010117130139 Kelas: CSariNo ratings yet
- Emotion As Risk FactorDocument9 pagesEmotion As Risk FactorMirza BangunNo ratings yet
- Health and Quality of Life OutcomesDocument11 pagesHealth and Quality of Life OutcomesAoikiji KuzanNo ratings yet
- Subhealth: Definition, Criteria For Diagnosis and Potential Prevalence in The Central Region of ChinaDocument8 pagesSubhealth: Definition, Criteria For Diagnosis and Potential Prevalence in The Central Region of ChinaLuis Javier CastroNo ratings yet
- The Secrets You Should Know About Sexual Medicine; Part One; Obesity and Sexual DysfunctionFrom EverandThe Secrets You Should Know About Sexual Medicine; Part One; Obesity and Sexual DysfunctionNo ratings yet
- Purpose in Life and Use of Preventive Health Care Services: A B C DDocument6 pagesPurpose in Life and Use of Preventive Health Care Services: A B C Dadilla kusumaNo ratings yet
- Fitness or Activity Blair 2001Document21 pagesFitness or Activity Blair 2001AisyahMKNo ratings yet
- Diet in DepressionDocument7 pagesDiet in Depressionanwaarft123No ratings yet
- NIH Public Access: Author ManuscriptDocument17 pagesNIH Public Access: Author ManuscriptaiusvestaNo ratings yet
- Vegetarian Diet and Mental Disorders: Results From A Representative Community SurveyDocument10 pagesVegetarian Diet and Mental Disorders: Results From A Representative Community SurveydeboracrpNo ratings yet
- The Relationship Between Life Satisfaction and Health BehaviorsDocument10 pagesThe Relationship Between Life Satisfaction and Health BehaviorsJesus GuerreroNo ratings yet
- Hostility and The Metabolic Syndrome in Older Males: The Normative Aging StudyDocument10 pagesHostility and The Metabolic Syndrome in Older Males: The Normative Aging StudymrclpppNo ratings yet
- Angermayr Et Al. - 2010 - Multifactorial Lifestyle Interventions in The PrimDocument16 pagesAngermayr Et Al. - 2010 - Multifactorial Lifestyle Interventions in The Prim4kfzzagyveNo ratings yet
- Research ArticleDocument12 pagesResearch ArticleSukmaNo ratings yet
- Physical Health Assessment and Cardiometabolic Monitoring Practices Across Three Adult Mental Health Inpatient Units - A Retrospective Cohort StudyDocument13 pagesPhysical Health Assessment and Cardiometabolic Monitoring Practices Across Three Adult Mental Health Inpatient Units - A Retrospective Cohort StudyEshetu WondimuNo ratings yet
- How Happiness and Positive Emotions Can Improve Health and LongevityDocument65 pagesHow Happiness and Positive Emotions Can Improve Health and LongevityPuteri Nur TriyandiniNo ratings yet
- Health Related Quality of Life, Depression and Anxiety Among People With Type 2 Diabetes Mellitus in BangladeshDocument26 pagesHealth Related Quality of Life, Depression and Anxiety Among People With Type 2 Diabetes Mellitus in BangladeshGhanva KhanNo ratings yet
- Religiosity Spirituality and Physiological Markers of Health - shattuck 2018Document20 pagesReligiosity Spirituality and Physiological Markers of Health - shattuck 2018Mércia FiuzaNo ratings yet
- Tdah 2Document11 pagesTdah 2Roberto Alexis Molina CampuzanoNo ratings yet
- Overweight and Obesity Associated With Higher Depression Prevalence in Adults: A Systematic Review and Meta-AnalysisDocument12 pagesOverweight and Obesity Associated With Higher Depression Prevalence in Adults: A Systematic Review and Meta-AnalysisLev FyodorNo ratings yet
- Nutrients 11 00148Document11 pagesNutrients 11 00148Putri N.AprilliaNo ratings yet
- Ijerph 14030240Document17 pagesIjerph 14030240Miss LeslieNo ratings yet
- Pigłowska 2016Document8 pagesPigłowska 2016Sam Steven Hernandez JañaNo ratings yet
- A Randomised Controlled Trial of Dietary Improvement For Adults With Major Depression (The SMILES' Trial)Document13 pagesA Randomised Controlled Trial of Dietary Improvement For Adults With Major Depression (The SMILES' Trial)agalbimaNo ratings yet
- Healthy Happiness: Effects of Happiness On Physical Health and The Consequences For Preventive Health CareDocument26 pagesHealthy Happiness: Effects of Happiness On Physical Health and The Consequences For Preventive Health CareAnonymous Fqa80pKNo ratings yet
- Leptin, abdominal obesity and risk of depression onset in older menDocument15 pagesLeptin, abdominal obesity and risk of depression onset in older menandinitaaaNo ratings yet
- Research ArticleDocument8 pagesResearch ArticleWan-FeiKhawNo ratings yet
- Body Mass IndexDocument6 pagesBody Mass Indexayu yuliantiNo ratings yet
- Switch Olanzapin Ke RisperidonDocument10 pagesSwitch Olanzapin Ke RisperidonAnonymous Ca0YyWNnVNo ratings yet
- Antidepressants and Health-Related Quality of Life For Patients With DepressionDocument14 pagesAntidepressants and Health-Related Quality of Life For Patients With Depressionjohndoe691488No ratings yet
- Preventive Medicine: Charlotta Pisinger, Ulla Toft, Mette Aadahl, Charlotte Glümer, Torben JørgensenDocument6 pagesPreventive Medicine: Charlotta Pisinger, Ulla Toft, Mette Aadahl, Charlotte Glümer, Torben JørgensenIgor BatovNo ratings yet
- Final Research ProjectDocument21 pagesFinal Research Projectapi-339312954No ratings yet
- Diabetes and Exercise: From Pathophysiology to Clinical ImplementationFrom EverandDiabetes and Exercise: From Pathophysiology to Clinical ImplementationJane E. B. Reusch, MDNo ratings yet
- Aging YeniDocument19 pagesAging YeniDr.Serkan SenerNo ratings yet
- Kuczmarski 2010Document7 pagesKuczmarski 2010Alejandra LópezNo ratings yet
- 2013 Best Prac Endoc - Impacto de La Obesidad en La Calidad de VidaDocument8 pages2013 Best Prac Endoc - Impacto de La Obesidad en La Calidad de VidaAndrew Paul Zamora HuancasNo ratings yet
- BJC 2015310 ADocument12 pagesBJC 2015310 AJuliana SoaresNo ratings yet
- PNAS 2016 McClintock E3071 80Document10 pagesPNAS 2016 McClintock E3071 80Karina Alejandra GarcíaNo ratings yet
- Dietary Diversity and Healthy Aging - A Prospective Study 2021Document15 pagesDietary Diversity and Healthy Aging - A Prospective Study 2021Kelly DickinsonNo ratings yet
- Metabolic Syndrome Risk Factors in Taiwanese AdultsDocument8 pagesMetabolic Syndrome Risk Factors in Taiwanese Adultsspringday_2004No ratings yet
- 10.1038@s41598 017 10775 3 PDFDocument8 pages10.1038@s41598 017 10775 3 PDFAlyssa LeuenbergerNo ratings yet
- Literature Review UpdatedDocument7 pagesLiterature Review Updatedapi-392259592No ratings yet
- PA and CM Risk Factor Young AdultDocument14 pagesPA and CM Risk Factor Young AdultMumtaz MaulanaNo ratings yet
- 06 - Chapter 1Document147 pages06 - Chapter 1pramodNo ratings yet
- Doc1Document11 pagesDoc1Sajal S.KumarNo ratings yet
- Ruben Rodriguez Essay 2 Final Draft Engl 2 RevisedDocument8 pagesRuben Rodriguez Essay 2 Final Draft Engl 2 Revisedapi-665390379No ratings yet
- Rodríguez-Monforte 2017 MS and Dietary PatternsDocument23 pagesRodríguez-Monforte 2017 MS and Dietary PatternsPaul SimononNo ratings yet
- U.S. Department of Health, Education, and Welfare, 1979 IOM, 1982Document14 pagesU.S. Department of Health, Education, and Welfare, 1979 IOM, 1982puskesmas beloNo ratings yet
- 2021-Young Adult Mental Health Sequelae of Eating and Body Image Disturbances in AdolescenceDocument9 pages2021-Young Adult Mental Health Sequelae of Eating and Body Image Disturbances in AdolescenceMarietta_MonariNo ratings yet
- Depression and Its Relationship To Physical Activity and ObesityDocument21 pagesDepression and Its Relationship To Physical Activity and ObesityAsdfghjklNo ratings yet
- Association Between A Comprehensive Movement Assesment and MetabolicallyDocument9 pagesAssociation Between A Comprehensive Movement Assesment and MetabolicallyzunigasanNo ratings yet
- Research Clinical 1 1Document18 pagesResearch Clinical 1 1api-459656816No ratings yet
- Assessment of College Students Awareness and Knowledge About Conditions Relevant To Metabolic SyndromeDocument15 pagesAssessment of College Students Awareness and Knowledge About Conditions Relevant To Metabolic SyndromeManimegalai SNo ratings yet
- ALS WordDocument4 pagesALS WordWahida AminNo ratings yet
- Psycho CardiologyDocument10 pagesPsycho Cardiologyciobanusimona259970No ratings yet
- Adhrnc Articl Simpl UnderstandDocument7 pagesAdhrnc Articl Simpl UnderstandMary Ann OquendoNo ratings yet
- Diabetik Dan KelainannyaDocument11 pagesDiabetik Dan Kelainannyalatifah zahrohNo ratings yet
- Ruben Rodriguez Essay 2 Final Draft Engl 2Document8 pagesRuben Rodriguez Essay 2 Final Draft Engl 2api-665390379No ratings yet
- TermoooDocument11 pagesTermoooJay-r Capate TanNo ratings yet
- ACS Sainsbury and Asda Merger Leaner 82Document26 pagesACS Sainsbury and Asda Merger Leaner 82FlareGBANo ratings yet
- Akanānuru - Some Poems (2012 - 10 - 29 02 - 55 - 25 UTC)Document9 pagesAkanānuru - Some Poems (2012 - 10 - 29 02 - 55 - 25 UTC)Ravi SoniNo ratings yet
- Edwin A. Winckler. Political AnthropologyDocument87 pagesEdwin A. Winckler. Political AnthropologyGabriela Herrera MonrroyNo ratings yet
- Galeo Wa430-6 PDFDocument1,612 pagesGaleo Wa430-6 PDFWalter100% (1)
- Telemecanique Integral 32 Motor StarterDocument52 pagesTelemecanique Integral 32 Motor StarterJaime IxtaNo ratings yet
- Profession Jokes - DoctorsDocument10 pagesProfession Jokes - DoctorssagararlaNo ratings yet
- Hypothesis of The Origin of LanguageDocument6 pagesHypothesis of The Origin of LanguageJefferson KagiriNo ratings yet
- Iberchem - French: Code Item Name Code Item Name 35000 7600Document2 pagesIberchem - French: Code Item Name Code Item Name 35000 7600Noor AshrafiNo ratings yet
- LA36300 Circuit Breaker Data SheetDocument2 pagesLA36300 Circuit Breaker Data SheetALEJANDRO DOMINGUEZNo ratings yet
- Obadiah Final Manuscript 16 01Document50 pagesObadiah Final Manuscript 16 01Zenaida FeliasNo ratings yet
- Those Who Serve - Stephen Melillo (Score)Document22 pagesThose Who Serve - Stephen Melillo (Score)Fernando RamiresNo ratings yet
- Teaching Plan: Objectives Identified Problems/Concerns Activities Evaluation Student Nurse Client/Family MemberDocument5 pagesTeaching Plan: Objectives Identified Problems/Concerns Activities Evaluation Student Nurse Client/Family MemberRaine SarmientoNo ratings yet
- Bar Code Label Requirements, Compatibility, and UsageDocument22 pagesBar Code Label Requirements, Compatibility, and Usagelarrylegend33No ratings yet
- B. Pharm.2nd 3rd 4th 2016-17Document8 pagesB. Pharm.2nd 3rd 4th 2016-17Mukesh TiwariNo ratings yet
- Crimean-Congo Hemorrhagic Fever ReviewDocument31 pagesCrimean-Congo Hemorrhagic Fever ReviewfaizalNo ratings yet
- XFGRRRDocument100 pagesXFGRRRAbchoNo ratings yet
- Parts List - KTZ411-63Document4 pagesParts List - KTZ411-63Mahmoud ElboraeNo ratings yet
- Bittersweet Tragedy - Melanie Martinez - LETRASDocument2 pagesBittersweet Tragedy - Melanie Martinez - LETRASFlávia FernandesNo ratings yet
- SHS 2023 Thinking Skills Practice Test QuestionsDocument32 pagesSHS 2023 Thinking Skills Practice Test Questionsvenkatesh113No ratings yet
- New Correlations For Predicting Two Phase Electrical SubmersibleDocument11 pagesNew Correlations For Predicting Two Phase Electrical SubmersibleNicolás Ruiz FuentesNo ratings yet
- Mobile C Arm PortfolioDocument6 pagesMobile C Arm PortfolioAri ReviantoNo ratings yet
- Module 2: Hematopoiesis I. General Principles of HematopoiesisDocument13 pagesModule 2: Hematopoiesis I. General Principles of HematopoiesisJane JapoleNo ratings yet
- Jaguar Land-Rover: A Customer Centric OrganizationDocument15 pagesJaguar Land-Rover: A Customer Centric OrganizationAnmol Shukla100% (1)
- Determination of Melting Point of An Organic CompoundDocument4 pagesDetermination of Melting Point of An Organic CompoundyteyetyeNo ratings yet
- LugeonDocument13 pagesLugeonRojan MaghsoodifarNo ratings yet
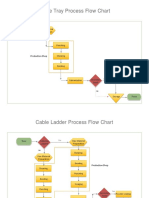
- Process Flow ChartDocument4 pagesProcess Flow Chartchacko chiramalNo ratings yet
- IOA Annual Report 2005Document18 pagesIOA Annual Report 2005matt30911No ratings yet
- Audi 6 3l w12 Fsi EngineDocument4 pagesAudi 6 3l w12 Fsi EngineMarlon100% (54)
- Northridge E250pDocument23 pagesNorthridge E250pVion VionNo ratings yet