You might also like
- Disk HerniationDocument27 pagesDisk HerniationDamiati78No ratings yet
- Cervical MyelopathyDocument18 pagesCervical MyelopathyRangga InktaenNdoek'sNo ratings yet
- Acute AppendicitisDocument36 pagesAcute AppendicitisOlivia CristieNo ratings yet
- Final PottsDocument60 pagesFinal Pottsharsh.chandane100% (6)
- DR - Rieva Kuliah 7 November - 2018Document38 pagesDR - Rieva Kuliah 7 November - 2018Nisrina100% (1)
- Datasheet For Voluson E6 bt17 002Document18 pagesDatasheet For Voluson E6 bt17 002muhammed kaletNo ratings yet
- Procedure for Phased Array and TOFD Ultrasonic Examination of Butt WeldsDocument40 pagesProcedure for Phased Array and TOFD Ultrasonic Examination of Butt Weldsrupam100% (6)
- Perthes Disease: by Dr. Abdul Karim Postgraduate Resident Orthopedic Surgery Pgmi/Lgh. Lahore PakistanDocument68 pagesPerthes Disease: by Dr. Abdul Karim Postgraduate Resident Orthopedic Surgery Pgmi/Lgh. Lahore Pakistandrakkashmiri50% (2)
- FRCR Physics MCQs in Clinical Radiology Exam 2 QDocument11 pagesFRCR Physics MCQs in Clinical Radiology Exam 2 QDr. BongaNo ratings yet
- 04 - Elements of EchocardiographyDocument56 pages04 - Elements of EchocardiographyMariana CabralNo ratings yet
- Self Assessment in Musculoskeletal Pathology X-raysFrom EverandSelf Assessment in Musculoskeletal Pathology X-raysRating: 5 out of 5 stars5/5 (2)
- Avascular NecrosisDocument8 pagesAvascular NecrosisBobyAnugrahNo ratings yet
- Legg Calvé Perthes DiseaseDocument11 pagesLegg Calvé Perthes DiseaseronnyNo ratings yet
- To 33B-1-1 01jan2013Document856 pagesTo 33B-1-1 01jan2013izmitlimonNo ratings yet
- Hip Disorders in Children: Postgraduate Orthopaedics SeriesFrom EverandHip Disorders in Children: Postgraduate Orthopaedics SeriesRating: 3 out of 5 stars3/5 (2)
- Legg Calve PerthesDocument93 pagesLegg Calve PerthesAkshay LakraNo ratings yet
- Dr. Waqas Ayubian Notes For Step 3Document772 pagesDr. Waqas Ayubian Notes For Step 3Muhammad HammadNo ratings yet
- POTT's DISEASEDocument33 pagesPOTT's DISEASEJemimah A. Mangalindan100% (4)
- Legg-Calve'-Perthes Disease He National Osteonecrosis FoundationDocument5 pagesLegg-Calve'-Perthes Disease He National Osteonecrosis FoundationDanica May Corpuz Comia-EnriquezNo ratings yet
- Radiographic features of Perthes disease, DDH, AVN, OA hip and ANHDocument14 pagesRadiographic features of Perthes disease, DDH, AVN, OA hip and ANHEMIRZA NUR WICAKSONONo ratings yet
- Updateonevaluationand Treatmentofscoliosis: Ron El-Hawary,, Chukwudi ChukwunyerenwaDocument19 pagesUpdateonevaluationand Treatmentofscoliosis: Ron El-Hawary,, Chukwudi Chukwunyerenwacarla grauNo ratings yet
- Traumatic Spondyloptosis Resulting in Complete SCI Final RevDocument9 pagesTraumatic Spondyloptosis Resulting in Complete SCI Final RevSamuel WillyartoNo ratings yet
- Perthe's Disease Treatment and PrognosisDocument45 pagesPerthe's Disease Treatment and PrognosisAh ZhangNo ratings yet
- Legg CALVE PERVE DISEASEDocument7 pagesLegg CALVE PERVE DISEASEYussika FernandaNo ratings yet
- Osteonecrosis of The Femoral Head: Evaluation and TreatmentDocument10 pagesOsteonecrosis of The Femoral Head: Evaluation and TreatmentHector Ulises Quintanilla SotoNo ratings yet
- Legg-Calvé-Perthes Disease: Roberto E. Novo, DVM, DACVSDocument2 pagesLegg-Calvé-Perthes Disease: Roberto E. Novo, DVM, DACVSEdi BackyNo ratings yet
- From Toddler to Adolescence: Legg-Calve-Perthes DiseaseDocument4 pagesFrom Toddler to Adolescence: Legg-Calve-Perthes DiseaseGabriel MolinaNo ratings yet
- ScoliosisDocument11 pagesScoliosisLoredana GeorgescuNo ratings yet
- Pott's Disease Is A Presentation of ExtrapulmonaryDocument13 pagesPott's Disease Is A Presentation of ExtrapulmonaryJc HarharNo ratings yet
- Osteonecrosis of Femoral HeadDocument70 pagesOsteonecrosis of Femoral HeadStar CruiseNo ratings yet
- Empty Sella Syndrome: Continuing Education ActivityDocument8 pagesEmpty Sella Syndrome: Continuing Education Activityn2763288No ratings yet
- Exercise-Associated Numbness and Tingling in The Legs: For Editorial Comment See Page 1509Document4 pagesExercise-Associated Numbness and Tingling in The Legs: For Editorial Comment See Page 1509herpthederpNo ratings yet
- Slipped Capital Femoral Epiphysis: Vivek PandeyDocument30 pagesSlipped Capital Femoral Epiphysis: Vivek PandeyvivpanNo ratings yet
- Bony Lesions in Pediatric Acute LeukemiaDocument16 pagesBony Lesions in Pediatric Acute LeukemiaRani Henty NovitaNo ratings yet
- Chitty SkeletalDocument34 pagesChitty SkeletalAhmed H. Ali ElbestaweyNo ratings yet
- Descripon Viejita Pero BuenaDocument16 pagesDescripon Viejita Pero BuenaJorge Octavio Ibarra ChairezNo ratings yet
- Causes and Symptoms of Cervical SpondylosisDocument5 pagesCauses and Symptoms of Cervical SpondylosisMandyAoNo ratings yet
- Skeik Et Al 2015 - CirculatoryDocument5 pagesSkeik Et Al 2015 - Circulatorymattlight07No ratings yet
- Student Case of Girl With LumpDocument28 pagesStudent Case of Girl With LumpclikgoNo ratings yet
- Surgical Management of Cervical Myelopathy: Clinical EvaulationDocument10 pagesSurgical Management of Cervical Myelopathy: Clinical EvaulationBaharudin Yusuf RamadhaniNo ratings yet
- Legg-Calvé-Perthes Disease - An Overview With Recent LiteratureDocument10 pagesLegg-Calvé-Perthes Disease - An Overview With Recent LiteratureFranz BlacuttNo ratings yet
- Pictorial Essay: Radiographic Skeletal Changes in Sickle Cell AnemiaDocument6 pagesPictorial Essay: Radiographic Skeletal Changes in Sickle Cell AnemiaAustine OsaweNo ratings yet
- Cervical PainDocument4 pagesCervical PainRhomadhoni Ika PutraNo ratings yet
- Cauda Equina Syndrome: Signs, Symptoms, and Surgical TimingDocument35 pagesCauda Equina Syndrome: Signs, Symptoms, and Surgical TimingVamsi MohanNo ratings yet
- Muskulskletal RadiologiDocument35 pagesMuskulskletal RadiologiRuki HartawanNo ratings yet
- Coxa PlanaDocument3 pagesCoxa PlanaBer AnneNo ratings yet
- DR - O. K. A. SamuelsDocument76 pagesDR - O. K. A. Samuelsgdudex118811No ratings yet
- Cervical Spondylosis Background PathophysiologyDocument5 pagesCervical Spondylosis Background PathophysiologyhendrayatiranyNo ratings yet
- Cerebral Palsy - Beyond Hip DeformitiesDocument8 pagesCerebral Palsy - Beyond Hip DeformitiesmiguelpaillalefgutierrezNo ratings yet
- Mucopolysaccharidosis Type IVADocument31 pagesMucopolysaccharidosis Type IVALeidy Paola Gamboa GamboaNo ratings yet
- Avoiding Common Errors in The Emergency Department-801-1002Document200 pagesAvoiding Common Errors in The Emergency Department-801-1002Hernando CastrillónNo ratings yet
- Management of The Spine in Cerebral PalsyDocument7 pagesManagement of The Spine in Cerebral PalsyDitaAnggaraKusumaNo ratings yet
- DR Zameer Ali ST Stephen's HospitalDocument152 pagesDR Zameer Ali ST Stephen's Hospitalagnes trianaNo ratings yet
- Avascular Necrosis of Femoral HeadDocument50 pagesAvascular Necrosis of Femoral HeadStar CruiseNo ratings yet
- Anis's 4th Year ProjectDocument56 pagesAnis's 4th Year ProjectAnis Aziz AmalaniNo ratings yet
- Radiology Revision For MRCP IIDocument430 pagesRadiology Revision For MRCP IIMuntadher KareemNo ratings yet
- Acetabular Dysplasia in Adults - JBJSDocument3 pagesAcetabular Dysplasia in Adults - JBJSErnesto Ewertz MiquelNo ratings yet
- CoxaDocument9 pagesCoxaEmkhei GonzalesNo ratings yet
- Legg Calve Perthes Disease - RP's Ortho NotesDocument2 pagesLegg Calve Perthes Disease - RP's Ortho NotesSabari NathNo ratings yet
- Cauda Equina Syndrome: LSUHSC Neuroscience Student ClerkshipDocument32 pagesCauda Equina Syndrome: LSUHSC Neuroscience Student ClerkshipraraNo ratings yet
- Ficat and Arlet staging of hip AVNDocument6 pagesFicat and Arlet staging of hip AVNFernando Sugiarto0% (1)
- Coxa PlanaDocument3 pagesCoxa PlanacarolbeeeNo ratings yet
- Enfermedades LisosomalesDocument32 pagesEnfermedades LisosomalesJonathanOmarLaraAcevedoNo ratings yet
- West Indian Medical Journal: A Case of Pathological Rib Fractures: Focal Osteolysis or Osteoporosis?Document10 pagesWest Indian Medical Journal: A Case of Pathological Rib Fractures: Focal Osteolysis or Osteoporosis?IstianahNo ratings yet
- Posterior Circulation Stroke: Advances in Understanding and ManagementFrom EverandPosterior Circulation Stroke: Advances in Understanding and ManagementJong S. KimNo ratings yet
- Legg Calve PerthesDocument3 pagesLegg Calve PerthesDaniel OwenNo ratings yet
- Legg-Calve-Perthes DiseaseDocument2 pagesLegg-Calve-Perthes DiseaseEalsa CTNo ratings yet
- Lion Air Eticket Itinerary / ReceiptDocument0 pagesLion Air Eticket Itinerary / ReceiptAzhar ZulfikarNo ratings yet
- Tarian Tradisional Masyarakat Helong: Tari HopongDocument3 pagesTarian Tradisional Masyarakat Helong: Tari HopongEalsa CTNo ratings yet
- 1603 ECUBEi7 Web Catalogue ENG Low Sheet PDFDocument7 pages1603 ECUBEi7 Web Catalogue ENG Low Sheet PDFeduardoNo ratings yet
- Products Catalogue JUMPER 2015Document18 pagesProducts Catalogue JUMPER 2015dhirajkumar_1No ratings yet
- WS Emergency Echo SYMCARD 2022Document33 pagesWS Emergency Echo SYMCARD 2022IndRa KaBhuomNo ratings yet
- Historia de La NeurosonologiaDocument9 pagesHistoria de La NeurosonologiaEduardo RodriguezNo ratings yet
- ICD9CM2010Document666 pagesICD9CM2010Thyka MayasariNo ratings yet
- GE Logic7 Bt06Document16 pagesGE Logic7 Bt06ilias kaprosNo ratings yet
- Eco MSK 1Document7 pagesEco MSK 1Gabriela BichirNo ratings yet
- Tugas Translate UsgDocument408 pagesTugas Translate UsgHamdanSyarifNo ratings yet
- Logiq P Series: Make It Easy. Make It Your OwnDocument2 pagesLogiq P Series: Make It Easy. Make It Your OwnNam LeNo ratings yet
- Catalogo Aclaria Ax 8Document2 pagesCatalogo Aclaria Ax 8Soporte VitalNo ratings yet
- Specifications For An Ultrasound MachineDocument2 pagesSpecifications For An Ultrasound MachineTony starkNo ratings yet
- FCC 2018 Mopup Vacancy 270219Document50 pagesFCC 2018 Mopup Vacancy 270219Anish H DaveNo ratings yet
- Manual Phased Array Ultrasonic Technique For Weld ApplicationDocument7 pagesManual Phased Array Ultrasonic Technique For Weld ApplicationphanthanhhungNo ratings yet
- Top NABH and Non-NABH Hospitals and Eye Centres in BangaloreDocument53 pagesTop NABH and Non-NABH Hospitals and Eye Centres in BangaloremamuhydNo ratings yet
- Common Probe FailuresDocument18 pagesCommon Probe FailuresEuris Otilio Dominguez AmadisNo ratings yet
- Acoustic Lens Improves Superficial In-Plane Ultrasound-Guided ProceduresDocument6 pagesAcoustic Lens Improves Superficial In-Plane Ultrasound-Guided ProceduresHarm ScholtenNo ratings yet
- Philips Iu22 BrochureDocument16 pagesPhilips Iu22 BrochurejamesNo ratings yet
- Disinfectants and Cleaning Solutions For Ultrasound Systems and Transducers - 453562014061a - en-US PDFDocument52 pagesDisinfectants and Cleaning Solutions For Ultrasound Systems and Transducers - 453562014061a - en-US PDFIvan CvasniucNo ratings yet
- Experimental Thermal and Fluid Science: SciencedirectDocument12 pagesExperimental Thermal and Fluid Science: Sciencedirectgokul mgkNo ratings yet
- TDS - Fischerscope UMP20!40!100-150Document4 pagesTDS - Fischerscope UMP20!40!100-150srpati_55555No ratings yet
- ALPINION Company Profile - ENG - F - 20170807Document28 pagesALPINION Company Profile - ENG - F - 20170807Mohammad NasriNo ratings yet
- Fbs 502touch LR Sales Lit 050913Document3 pagesFbs 502touch LR Sales Lit 050913api-221020032No ratings yet
- DIPSI GuidelinesDocument7 pagesDIPSI GuidelinesvinaypharmNo ratings yet
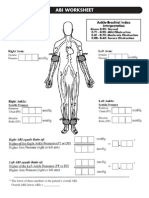
- Abi SheetsDocument2 pagesAbi Sheetszaky soewandi0% (1)