You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Civil Engineering Materials by Nagaratnam SivakuganDocument446 pagesCivil Engineering Materials by Nagaratnam SivakuganMario Trotea100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Identification of Textile FibersDocument41 pagesIdentification of Textile Fibersnitishkohli94% (36)
- 29 1.1 Stability Workshop ICH Q1AR2 CDocument60 pages29 1.1 Stability Workshop ICH Q1AR2 Celektron2010No ratings yet
- Future Journal of Pharmaceutical SciencesDocument13 pagesFuture Journal of Pharmaceutical Scienceselektron2010No ratings yet
- MGDocument12 pagesMGelektron2010No ratings yet
- Sindrome LumbociaticoDocument23 pagesSindrome Lumbociaticoelektron2010No ratings yet
- 0777 Ondrugdelivery Oral Drug Delivery July 2012 Low ResDocument24 pages0777 Ondrugdelivery Oral Drug Delivery July 2012 Low Reselektron2010No ratings yet
- 1-7 Manufacturing BasicsDocument29 pages1-7 Manufacturing Basicselektron2010No ratings yet
- Dgradcn Aaia AgiosDocument3 pagesDgradcn Aaia Agioselektron2010No ratings yet
- Car Box I Metil CelulosaDocument30 pagesCar Box I Metil Celulosaelektron2010No ratings yet
- T S P and PceduresDocument5 pagesT S P and Pcedureselektron2010No ratings yet
- Napr InterDocument8 pagesNapr Interelektron2010No ratings yet
- Testing Sieves Principles and Procedures PDFDocument24 pagesTesting Sieves Principles and Procedures PDFelektron2010No ratings yet
- Suon Lacn SteaDocument10 pagesSuon Lacn Steaelektron2010No ratings yet
- Market Structure, R&D and Advertising in The Pharmaceutical IndustryDocument27 pagesMarket Structure, R&D and Advertising in The Pharmaceutical Industryelektron2010No ratings yet
- A New Look at The Returns and Risks To Pharmaceutical R&DDocument19 pagesA New Look at The Returns and Risks To Pharmaceutical R&Delektron2010No ratings yet
- Chapter - 1: 1.1 GeneralDocument57 pagesChapter - 1: 1.1 GeneralMAHEN DRANNo ratings yet
- Heat Exchanger DesignDocument2 pagesHeat Exchanger DesignAmit Sharma ParasharNo ratings yet
- 23.01.24 - SR - STAR CO-SC (MODEL-A, B&C) - Jee - Main - GTM-25 (N) - QPDocument20 pages23.01.24 - SR - STAR CO-SC (MODEL-A, B&C) - Jee - Main - GTM-25 (N) - QPManju ManuNo ratings yet
- SMAW Module 2Document10 pagesSMAW Module 2Mclawrence SaquingNo ratings yet
- Bab 6 Makromolekul: Monomer POL I MerDocument3 pagesBab 6 Makromolekul: Monomer POL I Merburneracc121No ratings yet
- High Temperature SteelDocument5 pagesHigh Temperature Steelsathyadevi konnurNo ratings yet
- Cement Process PDFDocument36 pagesCement Process PDFAstha Yadav100% (3)
- Zero OrderDocument11 pagesZero Ordermahatir muhammadNo ratings yet
- AssignmentDocument2 pagesAssignmentsilverstonerocky0No ratings yet
- Effect of Boron and Carbon Addition On Microstructure and Mec 2015 MaterialsDocument14 pagesEffect of Boron and Carbon Addition On Microstructure and Mec 2015 Materialsnarayananx5No ratings yet
- Pre-Lab ReportDocument6 pagesPre-Lab ReportTintin Brusola SalenNo ratings yet
- Detailed Notes - Topic 10 Equilibrium I - Edexcel Chemistry A LevelDocument4 pagesDetailed Notes - Topic 10 Equilibrium I - Edexcel Chemistry A LevelLulwa KhaskiehNo ratings yet
- Chemcure - 15Document2 pagesChemcure - 15ICPL-RWPNo ratings yet
- ISUD 6 ProceedingsDocument192 pagesISUD 6 ProceedingsManea GrosuNo ratings yet
- 05.SOP For Storage and Use of Reagents & ChemicalsDocument4 pages05.SOP For Storage and Use of Reagents & ChemicalsBejoy Karim75% (4)
- Chapter 3Document80 pagesChapter 3Ezzati AzizNo ratings yet
- Bungard Line Proposals E 09Document12 pagesBungard Line Proposals E 09Cristian FernandezNo ratings yet
- CHEE2001 Week 2 Tutorial SheetDocument2 pagesCHEE2001 Week 2 Tutorial SheetMuntaha ManzoorNo ratings yet
- C15 Notes CH2 StoichiometryDocument5 pagesC15 Notes CH2 StoichiometryArnieNo ratings yet
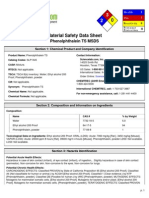
- MSDS PhenolphthaleinDocument6 pagesMSDS PhenolphthaleinAstri Aisyah RahmiNo ratings yet
- Historical Timeline of The AtomDocument19 pagesHistorical Timeline of The AtomHisagi ShuheiNo ratings yet
- Electrolyte Turns On The Solar Cell: 2009 Project SummaryDocument1 pageElectrolyte Turns On The Solar Cell: 2009 Project SummaryAshu SarasNo ratings yet
- Optimization Process of Biodiesel Production With Ultrasound Assisted by Using Central Composite Design MethodsDocument47 pagesOptimization Process of Biodiesel Production With Ultrasound Assisted by Using Central Composite Design MethodsMiftahFakhriansyahNo ratings yet
- Luff SchoorlDocument13 pagesLuff Schoorlmarijuana.hesNo ratings yet
- Irrigation in EndodonticsDocument157 pagesIrrigation in Endodonticsjoel devarajNo ratings yet
- Anthranilic Acid Chemical PropertiesDocument3 pagesAnthranilic Acid Chemical PropertiesDanNo ratings yet
- Carbothane 134 Series PDS Sept 2012Document2 pagesCarbothane 134 Series PDS Sept 2012salamrefighNo ratings yet
- Ch8651 Mass Transfer-Ii Unit IDocument22 pagesCh8651 Mass Transfer-Ii Unit ISherly ThomasNo ratings yet