You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Practical Power Plant Engineering A Guide For Early Career Engineers PDFDocument652 pagesPractical Power Plant Engineering A Guide For Early Career Engineers PDFsahli medNo ratings yet
- MKF Tool HelpDocument6 pagesMKF Tool HelpRob GoetzNo ratings yet
- Anais Nin - Under A Glass Bell-Pages-29-32 WordDocument6 pagesAnais Nin - Under A Glass Bell-Pages-29-32 WordArmina MNo ratings yet
- Module6 EngDocument29 pagesModule6 Engmega suryaNo ratings yet
- Module D Counselling44Document76 pagesModule D Counselling44Endang Susilowati NNo ratings yet
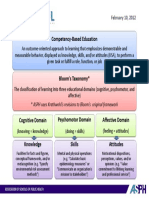
- Competency-Based Education: ASPH Uses Krathwohl's Revisions To Bloom's Original FrameworkDocument1 pageCompetency-Based Education: ASPH Uses Krathwohl's Revisions To Bloom's Original Frameworkmega suryaNo ratings yet
- Module4 EngDocument16 pagesModule4 Engmega suryaNo ratings yet
- Module1 Eng PDFDocument24 pagesModule1 Eng PDFmega suryaNo ratings yet
- R428 ICM 2011 Global Standards For Midwifery Education 2010 Companion Guidelines ENGDocument26 pagesR428 ICM 2011 Global Standards For Midwifery Education 2010 Companion Guidelines ENGmega suryaNo ratings yet
- The Midwifery CurriculumDocument41 pagesThe Midwifery Curriculummega surya100% (1)
- ICM Essential Competencies For Basic Midwifery Practice 2010, Revised 2013Document19 pagesICM Essential Competencies For Basic Midwifery Practice 2010, Revised 2013ayu_pieterNo ratings yet
- Future Dusk Portfolio by SlidesgoDocument40 pagesFuture Dusk Portfolio by SlidesgoNATALIA ALSINA MARTINNo ratings yet
- Eco 407Document4 pagesEco 407LUnweiNo ratings yet
- Stability Result 15275 MT - Initial StowageDocument1 pageStability Result 15275 MT - Initial StowageLife with Our planetNo ratings yet
- Meditation On God's WordDocument26 pagesMeditation On God's WordBeghin BoseNo ratings yet
- LESSON 6 Perfect TensesDocument4 pagesLESSON 6 Perfect TensesAULINO JÚLIONo ratings yet
- Description of Medical Specialties Residents With High Levels of Workplace Harassment Psychological Terror in A Reference HospitalDocument16 pagesDescription of Medical Specialties Residents With High Levels of Workplace Harassment Psychological Terror in A Reference HospitalVictor EnriquezNo ratings yet
- G.R. No. 201354 September 21, 2016Document11 pagesG.R. No. 201354 September 21, 2016Winston YutaNo ratings yet
- Akhbar Al Fuqaha Narration - Non Raful Yadayn From Ibn Umar - Reply To Zubair Ali ZaiDocument15 pagesAkhbar Al Fuqaha Narration - Non Raful Yadayn From Ibn Umar - Reply To Zubair Ali ZaiAbdullah YusufNo ratings yet
- Donna Haraway - A Cyborg Manifesto - An OutlineDocument2 pagesDonna Haraway - A Cyborg Manifesto - An OutlineKirill RostovtsevNo ratings yet
- Literacy Block Lesson PlanDocument5 pagesLiteracy Block Lesson Planapi-286592038No ratings yet
- BuildingBotWithWatson PDFDocument248 pagesBuildingBotWithWatson PDFjavaarchNo ratings yet
- How To Read A Research PaperDocument16 pagesHow To Read A Research PaperHena Afridi100% (1)
- Organisational Behaviour - II India Yamaha Motors Interim PPT (Download To View Full Presentation)Document28 pagesOrganisational Behaviour - II India Yamaha Motors Interim PPT (Download To View Full Presentation)mahtaabkNo ratings yet
- Persuasive SpeechDocument2 pagesPersuasive SpeechAngel Zachary RayyanNo ratings yet
- Mindfulness: Presented by Joshua Green, M.S. Doctoral Intern at Umaine Counseling CenterDocument12 pagesMindfulness: Presented by Joshua Green, M.S. Doctoral Intern at Umaine Counseling CenterLawrence MbahNo ratings yet
- Correct Translation of 2-16Document19 pagesCorrect Translation of 2-16muhammad_zubair708110No ratings yet
- Utsourcing) Is A Business: Atty. Paciano F. Fallar Jr. SSCR-College of Law Some Notes OnDocument9 pagesUtsourcing) Is A Business: Atty. Paciano F. Fallar Jr. SSCR-College of Law Some Notes OnOmar sarmiento100% (1)
- Quality of Life After Functional Endoscopic Sinus Surgery in Patients With Chronic RhinosinusitisDocument15 pagesQuality of Life After Functional Endoscopic Sinus Surgery in Patients With Chronic RhinosinusitisNarendraNo ratings yet
- Chapter 8 Review QuestionsDocument2 pagesChapter 8 Review QuestionsSouthernGurl99No ratings yet
- Simple Past TenseDocument6 pagesSimple Past Tenseanggun muslimahNo ratings yet
- M40 Mix DesignDocument2 pagesM40 Mix DesignHajarath Prasad Abburu100% (1)
- Suicide Prevention BrochureDocument2 pagesSuicide Prevention Brochureapi-288157545No ratings yet
- Working With Regular Expressions: Prof. Mary Grace G. VenturaDocument26 pagesWorking With Regular Expressions: Prof. Mary Grace G. VenturaAngela BeatriceNo ratings yet
- Seerat Mujaddid Alf-e-Sani (Urdu)Document518 pagesSeerat Mujaddid Alf-e-Sani (Urdu)Talib Ghaffari100% (12)
- Portel's Value Chain AnalysisDocument3 pagesPortel's Value Chain AnalysisNivedNo ratings yet
- Foreign Policy During Mahathir EraDocument7 pagesForeign Policy During Mahathir EraMuhamad Efendy Jamhar0% (1)
- Flexural Design of Fiber-Reinforced Concrete Soranakom Mobasher 106-m52Document10 pagesFlexural Design of Fiber-Reinforced Concrete Soranakom Mobasher 106-m52Premalatha JeyaramNo ratings yet