You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Influence of Pontic Design On Speech With An Anterior Fixed Dental Prosthesis, A Clinical Study and Finite Element AnalysisDocument9 pagesInfluence of Pontic Design On Speech With An Anterior Fixed Dental Prosthesis, A Clinical Study and Finite Element AnalysisAsihPuspitaPutriNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- New Doc 2018-03-21 PDFDocument1 pageNew Doc 2018-03-21 PDFAsihPuspitaPutriNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- New Doc 2018-03-21Document1 pageNew Doc 2018-03-21AsihPuspitaPutriNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
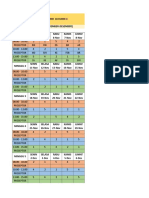
- JADWAL ASIH Copy 2Document2 pagesJADWAL ASIH Copy 2AsihPuspitaPutriNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Case Processing SummaryDocument22 pagesCase Processing SummaryAsihPuspitaPutriNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- New Doc 2018-03-21 PDFDocument1 pageNew Doc 2018-03-21 PDFAsihPuspitaPutriNo ratings yet
- New Doc 2018-04-16Document1 pageNew Doc 2018-04-16AsihPuspitaPutriNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Kegagalan GTC PDFDocument6 pagesKegagalan GTC PDFAsihPuspitaPutriNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Kegagalan GTC PDFDocument6 pagesKegagalan GTC PDFAsihPuspitaPutriNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Hand Lettering Letterform TemplateDocument1 pageHand Lettering Letterform TemplateMykovos0% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Pencetakan Dan Penatalaksanaan JaringanDocument8 pagesPencetakan Dan Penatalaksanaan JaringanAsihPuspitaPutriNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Jembatan AdhesifDocument5 pagesJembatan AdhesifAsihPuspitaPutriNo ratings yet
- New Doc 2017-11-22 PDFDocument25 pagesNew Doc 2017-11-22 PDFAsihPuspitaPutriNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- New Doc 2017-11-22Document25 pagesNew Doc 2017-11-22AsihPuspitaPutriNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- LesiDocument31 pagesLesiAsihPuspitaPutriNo ratings yet
- AttachmentDocument13 pagesAttachmentAsihPuspitaPutriNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hand Lettering Letterform TemplateDocument1 pageHand Lettering Letterform TemplateMykovos0% (1)
- (YNK) Introduction of CorporateDocument19 pages(YNK) Introduction of CorporateAsihPuspitaPutriNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Brush Lettering Practice Sheets DawnNicoleDesigns PDFDocument3 pagesBrush Lettering Practice Sheets DawnNicoleDesigns PDFAsihPuspitaPutriNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- A Possible Plant Adaptogen: Rhodiola RoseaDocument10 pagesA Possible Plant Adaptogen: Rhodiola RoseaAsihPuspitaPutriNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- ColorWorksheets DawnNicoleDesigns PDFDocument11 pagesColorWorksheets DawnNicoleDesigns PDFAsihPuspitaPutriNo ratings yet
- 1169-1410158654 EmulsiDocument5 pages1169-1410158654 EmulsiAsihPuspitaPutriNo ratings yet
- Breaking Emulsion (PDF)Document7 pagesBreaking Emulsion (PDF)adamsamodraNo ratings yet
- AttachmentDocument7 pagesAttachmentAsihPuspitaPutriNo ratings yet
- Israels JCDADocument13 pagesIsraels JCDATiffany MonicaNo ratings yet
- 1169-1410158654 EmulsiDocument5 pages1169-1410158654 EmulsiAsihPuspitaPutriNo ratings yet
- Israels JCDADocument13 pagesIsraels JCDATiffany MonicaNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- AttachmentDocument7 pagesAttachmentAsihPuspitaPutriNo ratings yet
- Dental Plaque PH Variation With Regular Soft Drink Diet Soft Drink and High Energy Drink An Iin Vivoi StudyDocument4 pagesDental Plaque PH Variation With Regular Soft Drink Diet Soft Drink and High Energy Drink An Iin Vivoi StudyAsihPuspitaPutriNo ratings yet
- Barbiturates and TranquilizerDocument4 pagesBarbiturates and TranquilizerSherryl ZamonteNo ratings yet
- TRIAZOLAMDocument4 pagesTRIAZOLAMEzequiel RosalesNo ratings yet
- Halcion Triazolam Tablets, USP CIV: DescriptionDocument14 pagesHalcion Triazolam Tablets, USP CIV: DescriptionAlberto JaramilloNo ratings yet
- CNS McqsDocument54 pagesCNS McqsMohammed KhalidNo ratings yet
- Benzodiazepines Rational UseDocument25 pagesBenzodiazepines Rational UseMila PetrovicNo ratings yet
- Week 11 Final Exam NURS 6630N ..Document17 pagesWeek 11 Final Exam NURS 6630N ..troillerdrippyNo ratings yet
- Sedative HypnoticsDocument41 pagesSedative HypnoticsPatrick Juacalla100% (2)
- CTC7 - Sample Chapter - Insomnia PDFDocument15 pagesCTC7 - Sample Chapter - Insomnia PDFFarid AhmedNo ratings yet
- Pharma Midterms CnsDocument67 pagesPharma Midterms CnsAL-NAZAERNo ratings yet
- Pharmacology Related To Psychiatric NursingDocument7 pagesPharmacology Related To Psychiatric NursingGlenn Daryll SantosNo ratings yet
- Assignment of Sedative HypnoticsDocument6 pagesAssignment of Sedative HypnoticsMae Lislie Canonigo - FloresNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Etextbook PDF For Juliens Primer of Drug Action A Comprehensive Guide To The Actions Uses and Side Effects of Psychoactive Drugs 14th EditioDocument62 pagesEtextbook PDF For Juliens Primer of Drug Action A Comprehensive Guide To The Actions Uses and Side Effects of Psychoactive Drugs 14th Editiobeverly.bustos487100% (42)
- Benzodiazepines 2022 Drug Fact Sheet - 1Document1 pageBenzodiazepines 2022 Drug Fact Sheet - 1Sharique KhanNo ratings yet
- The Darkside of Sleeping PillsDocument31 pagesThe Darkside of Sleeping PillsRitesh Kumar TripathiNo ratings yet
- Baby Katzung Second Shifting Reviewer PDFDocument13 pagesBaby Katzung Second Shifting Reviewer PDFJoanne Aluzan100% (1)
- Halcion WebDocument125 pagesHalcion WebdrkameshNo ratings yet
- Sedative-Hypnotic DrugsDocument8 pagesSedative-Hypnotic DrugsRoci ArceNo ratings yet
- Anti-Anxiety DrugsDocument3 pagesAnti-Anxiety DrugsClare100% (1)
- SedativeDocument15 pagesSedativeManul ShobujNo ratings yet
- Drug Cards CNSDocument23 pagesDrug Cards CNSChristine Schroeder100% (2)
- Mock Test 1 Part A Summer 2006Document53 pagesMock Test 1 Part A Summer 2006Alida Rautenbach0% (1)
- Benzo Conversion ChartDocument2 pagesBenzo Conversion ChartAl_CodaNo ratings yet
- Psychotropic MedicationsDocument17 pagesPsychotropic MedicationsMJ Torralba100% (1)
- Brand and Generic Medication Reference ListDocument6 pagesBrand and Generic Medication Reference ListAndi Dewi Pratiwi50% (2)
- Prescription For Addiction: UpdateDocument8 pagesPrescription For Addiction: Updateoptions1No ratings yet
- Digit Symbol Substitution Test: The Case For Sensitivity Over Specificity in Neuropsychological TestingDocument8 pagesDigit Symbol Substitution Test: The Case For Sensitivity Over Specificity in Neuropsychological TestingThe English TeacherNo ratings yet
- Overcoming Insomnia - Harvard Health PublicationsDocument5 pagesOvercoming Insomnia - Harvard Health PublicationssightbdNo ratings yet
- Sedative & HypnoticsDocument60 pagesSedative & HypnoticsDr Nilesh Patel100% (1)
- 1.4 CNS Drugs - Sedatives and Hypnotics - Dr. Rani Qasem 2014-2015Document23 pages1.4 CNS Drugs - Sedatives and Hypnotics - Dr. Rani Qasem 2014-2015Faisal FahadNo ratings yet
- Exam Autumn 2018 Questions and Answers PDFDocument418 pagesExam Autumn 2018 Questions and Answers PDFLauren SuttonNo ratings yet
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (38)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)