You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Autopsy of Baby WyllowDocument10 pagesAutopsy of Baby WyllowKOLD News 13100% (1)
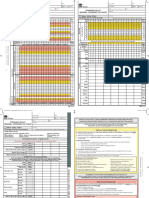
- SAGO AdultObsDocument2 pagesSAGO AdultObsTim BrownNo ratings yet
- Anatomy PDFDocument114 pagesAnatomy PDFkhualabear101100% (1)
- Hemomancer D&D 5e Homebrew ClassDocument11 pagesHemomancer D&D 5e Homebrew ClassAlexandre CrowNo ratings yet
- Reading Comprehension - English For Specific Purposes.-WitrianidocxDocument110 pagesReading Comprehension - English For Specific Purposes.-WitrianidocxAinun MaksuraNo ratings yet
- 2019-07-04 Calvert County TimesDocument24 pages2019-07-04 Calvert County TimesSouthern Maryland OnlineNo ratings yet
- (Đề thi có 04 trang) Thời gian làm bài: 60 phút không kể thời gian phát đềDocument5 pages(Đề thi có 04 trang) Thời gian làm bài: 60 phút không kể thời gian phát đềPhi VyNo ratings yet
- Hpc3 - The Menu and Its CourseDocument3 pagesHpc3 - The Menu and Its Coursemark danielNo ratings yet
- Differences in Social Hierarchies in Wild Vs Captive Chimp Communities: Cultural AdaptationDocument22 pagesDifferences in Social Hierarchies in Wild Vs Captive Chimp Communities: Cultural AdaptationntankardNo ratings yet
- The Red Smoothie Detox FactorDocument222 pagesThe Red Smoothie Detox FactorAndjela MiladinovicNo ratings yet
- VMR & IbsDocument7 pagesVMR & Ibsnovianti alfinaNo ratings yet
- Korrik Lore FinalDocument10 pagesKorrik Lore FinalGregory OsipovNo ratings yet
- 2013 ENDOCRINE PHARMACOLOGY Word Notes PDFDocument52 pages2013 ENDOCRINE PHARMACOLOGY Word Notes PDFNicole Opao100% (4)
- Fresh FishDocument23 pagesFresh FishARLENE MORADANo ratings yet
- Fathomless by Jackson PearceDocument37 pagesFathomless by Jackson PearceLittle, Brown Books for Young Readers100% (1)
- Spermatogenesis and FertilizationDocument21 pagesSpermatogenesis and FertilizationAyen FornollesNo ratings yet
- Pengaruh Umur Induk Dan Lama Penyimpanan Telur Terhadap Bobot Telur, Daya Tetas Dan Bobot Tetas Ayam Kedu Jengger MerahDocument4 pagesPengaruh Umur Induk Dan Lama Penyimpanan Telur Terhadap Bobot Telur, Daya Tetas Dan Bobot Tetas Ayam Kedu Jengger MerahKKN-T Gorontalo 2020No ratings yet
- Whats The SettingDocument2 pagesWhats The Settingapi-2428046300% (2)
- Cleft Lip and PalateDocument71 pagesCleft Lip and PalateMegha Sahni Grover75% (4)
- STD 12 English Board Question Paper Maharashtra BoardDocument22 pagesSTD 12 English Board Question Paper Maharashtra BoardTashvi KulkarniNo ratings yet
- WFRP - TalentsDocument8 pagesWFRP - TalentsIkkuhyuNo ratings yet
- Soal TOEFLDocument2 pagesSoal TOEFLArraya Eritha BarcelonaNo ratings yet
- Lecture Outline: See Separate Powerpoint Slides For All Figures and Tables Pre-Inserted Into Powerpoint Without NotesDocument61 pagesLecture Outline: See Separate Powerpoint Slides For All Figures and Tables Pre-Inserted Into Powerpoint Without NotesJharaNo ratings yet
- Ansci 1105 ReviewerDocument13 pagesAnsci 1105 ReviewerCj M SapadNo ratings yet
- Recurrent Vulvovaginal Candidiasis: Evidence-Based Pharmacy PracticeDocument4 pagesRecurrent Vulvovaginal Candidiasis: Evidence-Based Pharmacy PracticeRiddhi JainNo ratings yet
- Placental Abnormalities Normal Placenta: © Mary Andrea G. Agorilla, Ust-Con 2021 - 1Document3 pagesPlacental Abnormalities Normal Placenta: © Mary Andrea G. Agorilla, Ust-Con 2021 - 1Mary AgorillaNo ratings yet
- Една Кука Woollky Penguin Crochet Pattern by Babayaga EngDocument4 pagesЕдна Кука Woollky Penguin Crochet Pattern by Babayaga EngDiana BozhilovaNo ratings yet
- Project Report On Indian BirdsDocument9 pagesProject Report On Indian BirdsMridul kejriwal50% (2)
- English Practice Book 3.Document16 pagesEnglish Practice Book 3.GOALNo ratings yet
- ASDA Packet I-I (Part 1) PDFDocument46 pagesASDA Packet I-I (Part 1) PDFAbhi ThakkarNo ratings yet