You might also like
- Mehta 2011Document10 pagesMehta 2011Giulia AndreeaNo ratings yet
- Circulation Research-2015--e81-94Document40 pagesCirculation Research-2015--e81-94acNo ratings yet
- Mesenchymal Stromal Cells: Potential For Cardiovascular RepairDocument19 pagesMesenchymal Stromal Cells: Potential For Cardiovascular RepairardhanputraNo ratings yet
- 2019 Article 73Document10 pages2019 Article 73Radu AvramNo ratings yet
- Cell Tracking in Cardiac RepairDocument16 pagesCell Tracking in Cardiac RepairdeadcorpsesNo ratings yet
- (Guyette Et Al., 2015) Bioengineering Human Myocardium On Native Extracellular Matrix PDFDocument76 pages(Guyette Et Al., 2015) Bioengineering Human Myocardium On Native Extracellular Matrix PDFJulio dR AltavasNo ratings yet
- Rajala2011 PDFDocument13 pagesRajala2011 PDFInnakaNo ratings yet
- Thesis CardiomyocytesDocument8 pagesThesis Cardiomyocytesbsqfc4d5100% (2)
- 0271678x20953912 PDFDocument19 pages0271678x20953912 PDFHana Elsi putriNo ratings yet
- NIH Public AccessDocument18 pagesNIH Public AccessSofia BottiNo ratings yet
- Biochemical and Biophysical Research CommunicationsDocument7 pagesBiochemical and Biophysical Research CommunicationsGiulia AndreeaNo ratings yet
- Angoulvant Et Al. - 2011 - Mesenchymal Stem Cell Conditioned Media Attenuates in Vitro and Ex Vivo Myocardial Reperfusion InjuryDocument8 pagesAngoulvant Et Al. - 2011 - Mesenchymal Stem Cell Conditioned Media Attenuates in Vitro and Ex Vivo Myocardial Reperfusion Injuryscribd mendeleyNo ratings yet
- A Simple, Cost-Effective But Highly Efficient System For Deriving Ventricular Cardiomyocytes From Human Pluripotent Stem CellsDocument13 pagesA Simple, Cost-Effective But Highly Efficient System For Deriving Ventricular Cardiomyocytes From Human Pluripotent Stem CellsBrachy ZhaoNo ratings yet
- Haem 2007 cxcr4 MSC HomingDocument8 pagesHaem 2007 cxcr4 MSC HomingoaifoiweuNo ratings yet
- Ijms 23 03482 v2Document26 pagesIjms 23 03482 v2Ravi Kant TripathiNo ratings yet
- Vascular Organoids. Are We Enteringa New Area of Cardiometabolic Research - Cooper2019Document3 pagesVascular Organoids. Are We Enteringa New Area of Cardiometabolic Research - Cooper2019Shield YggdrasilNo ratings yet
- SCCAA 7820 Mesenchymal Stem Cells in The Treatment of Ischemic Stroke 111110Document7 pagesSCCAA 7820 Mesenchymal Stem Cells in The Treatment of Ischemic Stroke 111110Nur FitriahNo ratings yet
- MachalDocument5 pagesMachalMinh Vương NguyễnNo ratings yet
- UntitledDocument3 pagesUntitledNida MasroorNo ratings yet
- Cerebral Perfusion Simulation Using Realistically Generated Synthetic TreesDocument9 pagesCerebral Perfusion Simulation Using Realistically Generated Synthetic Treessunhao13287710014No ratings yet
- Collateral Benemerito2022Document11 pagesCollateral Benemerito2022Ivan BenemeritoNo ratings yet
- Chakravarty Et Al. - 2017 - ALLogeneic Heart STem Cells To Achieve Myocardial Regeneration (ALLSTAR) Trial Rationale and DesignDocument10 pagesChakravarty Et Al. - 2017 - ALLogeneic Heart STem Cells To Achieve Myocardial Regeneration (ALLSTAR) Trial Rationale and Designscribd mendeleyNo ratings yet
- Concise Review: Mesenchymal Stem Cells and Translational Medicine: Emerging IssuesDocument8 pagesConcise Review: Mesenchymal Stem Cells and Translational Medicine: Emerging IssuesLorenzo Maria CerviNo ratings yet
- Araya 2009. Localized Donor Cells in Brain of A Hunter Disease Patient After Cord Blood Stem Cell TransplantationDocument9 pagesAraya 2009. Localized Donor Cells in Brain of A Hunter Disease Patient After Cord Blood Stem Cell TransplantationBoNo ratings yet
- Cell Therapy in Patients With Critical Limb IschemiaDocument27 pagesCell Therapy in Patients With Critical Limb IschemiaAsep HrNo ratings yet
- Cetin 2016Document10 pagesCetin 2016Della Puspita SariNo ratings yet
- Isolation, Characterization, and Differentiation of Cardiac Stem CellsDocument7 pagesIsolation, Characterization, and Differentiation of Cardiac Stem CellsHadjer RezigNo ratings yet
- Data CollectionDocument9 pagesData Collectionapi-512131053No ratings yet
- Stem Cells For Myocardial Repair: Oren Caspi and Lior GepsteinDocument12 pagesStem Cells For Myocardial Repair: Oren Caspi and Lior Gepsteinandikaagus13No ratings yet
- Cell Therapy May Reduce Heart Failure After Acute Myocardial InfarctionDocument17 pagesCell Therapy May Reduce Heart Failure After Acute Myocardial InfarctionoswalpNo ratings yet
- CD96 is a Leukemic Stem Cell-specific Marker in HuDocument7 pagesCD96 is a Leukemic Stem Cell-specific Marker in HuLuis Alberto Sanchez VilelaNo ratings yet
- Therapeutic Cardiac Patches: BY Leah Sabu: 1Ms20Bt026 VIVEK T.R: 1MS20BT060Document16 pagesTherapeutic Cardiac Patches: BY Leah Sabu: 1Ms20Bt026 VIVEK T.R: 1MS20BT060Vivek TRNo ratings yet
- mainDocument8 pagesmainAxel MendozaNo ratings yet
- JCDR 9 OC09Document5 pagesJCDR 9 OC09Amrita JenaNo ratings yet
- Stemcells 2006-0409Document9 pagesStemcells 2006-0409dupuytrenNo ratings yet
- Baj Krzyworzeka (2002)Document10 pagesBaj Krzyworzeka (2002)Sitara AkbarNo ratings yet
- Original Article - Afterload Promotes Maturation of Human Induced Pluripotent Stem Cell DerivedDocument49 pagesOriginal Article - Afterload Promotes Maturation of Human Induced Pluripotent Stem Cell DerivedrizalalhasNo ratings yet
- Canonical transient receptor potential 6 channel deficiency promotes smooth muscle cells dedifferentiation and increased proliferation after arterial injuryDocument26 pagesCanonical transient receptor potential 6 channel deficiency promotes smooth muscle cells dedifferentiation and increased proliferation after arterial injurydiego.battiatoNo ratings yet
- 5 - Reticulated Platelets - Clinical Application and Future PerspectivesDocument13 pages5 - Reticulated Platelets - Clinical Application and Future PerspectivesnivmastNo ratings yet
- AJP Heart and Circulatory Physiology Volume 287 Issue 2 2004 (Doi 10.1152 - Ajpheart.01247.2003) Hodgson, D. M. - Stable Benefit of EmbryonDocument10 pagesAJP Heart and Circulatory Physiology Volume 287 Issue 2 2004 (Doi 10.1152 - Ajpheart.01247.2003) Hodgson, D. M. - Stable Benefit of EmbryonArini Dwi NastitiNo ratings yet
- Cancer 1Document8 pagesCancer 1JoseRodrigoSuarezCamposNo ratings yet
- Response NIHcommonfundDocument3 pagesResponse NIHcommonfundJames ParsonsNo ratings yet
- JMCC2003_YoshidaDocument23 pagesJMCC2003_Yoshidaslmkyl1805No ratings yet
- Stem Cell For Cardiac RepairDocument9 pagesStem Cell For Cardiac RepairAdi WijayantoNo ratings yet
- Role of The Extracellular Matrix in Cell-CellDocument3 pagesRole of The Extracellular Matrix in Cell-CellNicolásNo ratings yet
- Sel Mesenkim 4Document10 pagesSel Mesenkim 4Ida Ifan YulianaNo ratings yet
- Liu2007 Sox17Document7 pagesLiu2007 Sox17iulia andreeaNo ratings yet
- CRISPR/Cas9 Mediated Gene Correction Ameliorates Abnormal Phenotypes in Spinocerebellar Ataxia Type 3 Patient-Derived Induced Pluripotent Stem CellsDocument13 pagesCRISPR/Cas9 Mediated Gene Correction Ameliorates Abnormal Phenotypes in Spinocerebellar Ataxia Type 3 Patient-Derived Induced Pluripotent Stem CellsTamara MuñozNo ratings yet
- Reticulated Platelets - Clinical Application and FDocument13 pagesReticulated Platelets - Clinical Application and Ftufis02No ratings yet
- Biochemical and Biophysical Research CommunicationsDocument10 pagesBiochemical and Biophysical Research Communications马三强No ratings yet
- Shuyuan Guo, Yusen Zhang, Yanmin Zhang, Fanhua Meng, Minghua Li, Zhendong Yu, Yun Chen, and Guanghui CuiDocument14 pagesShuyuan Guo, Yusen Zhang, Yanmin Zhang, Fanhua Meng, Minghua Li, Zhendong Yu, Yun Chen, and Guanghui CuiEstefany CarrascalNo ratings yet
- STEM CELLS - 2009 - Schenk - Monocyte Chemotactic Protein 3 Is A Myocardial Mesenchymal Stem Cell Homing FactorDocument7 pagesSTEM CELLS - 2009 - Schenk - Monocyte Chemotactic Protein 3 Is A Myocardial Mesenchymal Stem Cell Homing FactorYasin DeveliogluNo ratings yet
- Review Article: Neuroprotective Effects of Stem Cells in Ischemic StrokeDocument7 pagesReview Article: Neuroprotective Effects of Stem Cells in Ischemic StrokesalmaNo ratings yet
- Bone Marrow Mesenchymal Stem Cell-Derived ExosomesDocument9 pagesBone Marrow Mesenchymal Stem Cell-Derived Exosomesiam_ca2No ratings yet
- UCM MSC Expansion Using Platelet LysateDocument1 pageUCM MSC Expansion Using Platelet LysateHanaNo ratings yet
- Mesenchymal Stem Cells in Cardiac Regeneration: A Detailed Progress Report of The Last 6 Years (2010 - 2015)Document25 pagesMesenchymal Stem Cells in Cardiac Regeneration: A Detailed Progress Report of The Last 6 Years (2010 - 2015)flying highNo ratings yet
- Tissue Engineering and Regeneration in Dentistry: Current StrategiesFrom EverandTissue Engineering and Regeneration in Dentistry: Current StrategiesRachel J. WaddingtonNo ratings yet
- Advances in Pluripotent Stem Cells: History, Mechanisms, Technologies, and ApplicationsDocument30 pagesAdvances in Pluripotent Stem Cells: History, Mechanisms, Technologies, and ApplicationsnembutalNo ratings yet
- 2018 Article 983Document13 pages2018 Article 983nembutalNo ratings yet
- Stem Cell and Gene Therapy for Cardiovascular DiseaseFrom EverandStem Cell and Gene Therapy for Cardiovascular DiseaseEmerson c. PerinNo ratings yet
- Ijms 18 00288 v2Document24 pagesIjms 18 00288 v2Cinsley GentillonNo ratings yet
- Proteomics Cardiac MetabDocument61 pagesProteomics Cardiac MetabCinsley GentillonNo ratings yet
- Bioactive-Lipids in Cardiac DiffDocument35 pagesBioactive-Lipids in Cardiac DiffCinsley GentillonNo ratings yet
- Bob Campbell-Proteomics HPSCDocument10 pagesBob Campbell-Proteomics HPSCCinsley GentillonNo ratings yet
- Amcas TipsDocument44 pagesAmcas TipsdaspammasterNo ratings yet
- High-Resolution Metabolomics of Occupational Exposure To TrichloroethyleneDocument11 pagesHigh-Resolution Metabolomics of Occupational Exposure To TrichloroethyleneCinsley GentillonNo ratings yet
- 2010 Glycolytic Network Restructuring Integral To The Energetics of Embryonic Stem Cell Cardiac DifferentiationDocument10 pages2010 Glycolytic Network Restructuring Integral To The Energetics of Embryonic Stem Cell Cardiac DifferentiationCinsley GentillonNo ratings yet
- 2016 Evidence For Intramyocardial Disruption of Lipid Metabolism and Increased Myocardial Ketone Utilization in Advanced Human Heart FailureDocument36 pages2016 Evidence For Intramyocardial Disruption of Lipid Metabolism and Increased Myocardial Ketone Utilization in Advanced Human Heart FailureCinsley GentillonNo ratings yet
- RNeasy Mini 0612Document80 pagesRNeasy Mini 0612xprakashNo ratings yet
- Acid-Base - FDocument14 pagesAcid-Base - FCinsley GentillonNo ratings yet
- The MCAT Physics BookDocument445 pagesThe MCAT Physics BookCinsley GentillonNo ratings yet
- TBR Writing1 OptDocument90 pagesTBR Writing1 OptMohamad ZriekNo ratings yet
- Aamc 4RDocument76 pagesAamc 4RBellony Sanders100% (2)
- TBR Writing1 OptDocument90 pagesTBR Writing1 OptMohamad ZriekNo ratings yet
- oExamKrackers MCAT Organic Chemistry BookDocument166 pagesoExamKrackers MCAT Organic Chemistry BookCinsley Gentillon100% (4)
- ProjectDocument86 pagesProjectrajuNo ratings yet
- Liquid Analysis v3 Powell-Cumming 2010 StanfordgwDocument28 pagesLiquid Analysis v3 Powell-Cumming 2010 StanfordgwErfanNo ratings yet
- How Do I Prepare For Public Administration For IAS by Myself Without Any Coaching? Which Books Should I Follow?Document3 pagesHow Do I Prepare For Public Administration For IAS by Myself Without Any Coaching? Which Books Should I Follow?saiviswanath0990100% (1)
- Political Engineering and Party Politics in Conflict-Prone SocietiesDocument18 pagesPolitical Engineering and Party Politics in Conflict-Prone SocietiesNashiba Dida-AgunNo ratings yet
- United Airlines Case Study: Using Marketing to Address External ChallengesDocument4 pagesUnited Airlines Case Study: Using Marketing to Address External ChallengesSakshiGuptaNo ratings yet
- Understanding 2006 PSAT-NMSQT ScoresDocument8 pagesUnderstanding 2006 PSAT-NMSQT ScorestacobeoNo ratings yet
- ElectricalDocument30 pagesElectricalketerNo ratings yet
- Siga-Cc1 12-22-2010Document6 pagesSiga-Cc1 12-22-2010Felipe LozanoNo ratings yet
- Barcelona Smart City TourDocument44 pagesBarcelona Smart City TourPepe JeansNo ratings yet
- Millennium Separation ReportDocument3 pagesMillennium Separation ReportAlexandra AkeNo ratings yet
- Handbook of Zen, Mindfulness and Spiritual Health PDFDocument324 pagesHandbook of Zen, Mindfulness and Spiritual Health PDFMatthew Grayson100% (3)
- Timber, PVCu and aluminium window and door hardware systemsDocument24 pagesTimber, PVCu and aluminium window and door hardware systemsOmul Fara NumeNo ratings yet
- FM 5130Document66 pagesFM 5130Aswini Kr KarmakarNo ratings yet
- Lateral capacity of pile in clayDocument10 pagesLateral capacity of pile in clayGeetha MaNo ratings yet
- Seismic Design of Steel Structures: Updates of Eurocode 8Document107 pagesSeismic Design of Steel Structures: Updates of Eurocode 8antonio111aNo ratings yet
- College of Physical Therapy Produces Skilled ProfessionalsDocument6 pagesCollege of Physical Therapy Produces Skilled ProfessionalsRia Mae Abellar SalvadorNo ratings yet
- TNTCL Cost Data 2021 22Document95 pagesTNTCL Cost Data 2021 22Akd DeshmukhNo ratings yet
- Internal Resistance and Matching in Voltage SourceDocument8 pagesInternal Resistance and Matching in Voltage SourceAsif Rasheed Rajput100% (1)
- GVB 1Document8 pagesGVB 1Aaron SylvestreNo ratings yet
- Inspection and Acceptance Report: Stock No. Unit Description QuantityDocument6 pagesInspection and Acceptance Report: Stock No. Unit Description QuantityAnj LeeNo ratings yet
- HHG4M - Lifespan Development Textbook Lesson 2Document95 pagesHHG4M - Lifespan Development Textbook Lesson 2Lubomira SucheckiNo ratings yet
- Boala Cronica Obstructive: BpocDocument21 pagesBoala Cronica Obstructive: BpocNicoleta IliescuNo ratings yet
- Hisar CFC - Approved DPRDocument126 pagesHisar CFC - Approved DPRSATYAM KUMARNo ratings yet
- Bhakti Trader Ram Pal JiDocument232 pagesBhakti Trader Ram Pal JiplancosterNo ratings yet
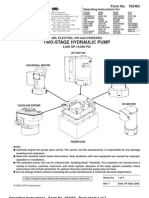
- Power Team PE55 ManualDocument13 pagesPower Team PE55 ManualTitanplyNo ratings yet
- Evolution Packet FinalDocument24 pagesEvolution Packet FinalJoaquinNo ratings yet
- Best Way To LearnDocument3 pagesBest Way To LearnRAMIZKHAN124No ratings yet
- Cell Selection ReselectionDocument35 pagesCell Selection ReselectionThiaguNo ratings yet
- Reversing a String in 8086 Micro Project ReportDocument4 pagesReversing a String in 8086 Micro Project ReportOm IngleNo ratings yet
- Integrating Therapeutic Play Into Nursing and Allied Health PracticeDocument214 pagesIntegrating Therapeutic Play Into Nursing and Allied Health PracticeIbrahim SabraNo ratings yet