You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- DCS800 Control PanelDocument9 pagesDCS800 Control PanelHenry Manzaneda100% (1)
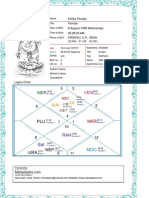
- Kritika Pandey (Kaushambi)Document15 pagesKritika Pandey (Kaushambi)nishink9No ratings yet
- Lesson Plan GagneDocument2 pagesLesson Plan Gagnechiew gin siongNo ratings yet
- Business Graphic CollectionDocument213 pagesBusiness Graphic CollectionHimansu Sekhar PradhanNo ratings yet
- Certifi Cati N: Salary DoesDocument8 pagesCertifi Cati N: Salary DoesGeeNo ratings yet
- C#Document3 pagesC#Dung RieuNo ratings yet
- STAT1008 Cheat SheetDocument1 pageSTAT1008 Cheat SheetynottripNo ratings yet
- ROBT308Lecture22Spring16 PDFDocument52 pagesROBT308Lecture22Spring16 PDFrightheartedNo ratings yet
- Mil STD 1316e Fuze DesignDocument25 pagesMil STD 1316e Fuze Designscorpion_l_81No ratings yet
- Chapter 3.3 - Cashflow and Continuous Compounding Sample ProblemsDocument14 pagesChapter 3.3 - Cashflow and Continuous Compounding Sample ProblemsArin ParkNo ratings yet
- Impact Force CalculationDocument3 pagesImpact Force CalculationphamvanlaiNo ratings yet
- Agarwal Packers ReviewDocument10 pagesAgarwal Packers ReviewAnonymous eDOS7RLyNo ratings yet
- BehaviourDocument16 pagesBehaviourIshita JainNo ratings yet
- Quiz1 ISDS361BDocument4 pagesQuiz1 ISDS361BAnh PhamNo ratings yet
- Autodesk Navisworks 2012 - Guia Do UsuárioDocument820 pagesAutodesk Navisworks 2012 - Guia Do UsuárioericfgNo ratings yet
- Fordyce MW 1983Document46 pagesFordyce MW 1983garbagepatchNo ratings yet
- 05 AccelerationDownIncline-2Document4 pages05 AccelerationDownIncline-2PeterNo ratings yet
- The Green Marketing "Revolution" - Is It WorthDocument12 pagesThe Green Marketing "Revolution" - Is It WorthAndrew SmithNo ratings yet
- 18-24 July 2009Document16 pages18-24 July 2009pratidinNo ratings yet
- Western Underground - HV and Ehv Cables-CmeDocument38 pagesWestern Underground - HV and Ehv Cables-CmeA. Hassan100% (2)
- Persepsi Masyarakat Terhadap Aplikasi Tiktok Sebagai Media Menurunkan Tingkat Stres Di Era Pandemi Covid-19Document7 pagesPersepsi Masyarakat Terhadap Aplikasi Tiktok Sebagai Media Menurunkan Tingkat Stres Di Era Pandemi Covid-19Syifa KhaerunnisaNo ratings yet
- Course 5 - Cooperative Principle and ImplicatureDocument6 pagesCourse 5 - Cooperative Principle and ImplicatureAnca Ionela ManoleNo ratings yet
- A Review of Shankuka's TheoryDocument14 pagesA Review of Shankuka's TheoryrajashreeNo ratings yet
- The Context Switch in FreeRTOS On A Cortex MDocument13 pagesThe Context Switch in FreeRTOS On A Cortex MKristof MulierNo ratings yet
- Understanding Work Conditioning and Work Hardening Programs For A Successful RTW 3 13 2014 NovaCare PDFDocument37 pagesUnderstanding Work Conditioning and Work Hardening Programs For A Successful RTW 3 13 2014 NovaCare PDFSitiSarah0% (1)
- Wolves, Witches, and Werewolves - Lycanthropy and Witchcraft From 1423 To 1700 PDFDocument28 pagesWolves, Witches, and Werewolves - Lycanthropy and Witchcraft From 1423 To 1700 PDFshotoshNo ratings yet
- Punjab UNiversity MSC Hons. School Physics ElectronicsDocument41 pagesPunjab UNiversity MSC Hons. School Physics ElectronicsDarrenLovelockNo ratings yet
- Documentation 040Document148 pagesDocumentation 040proxemicNo ratings yet
- Listening Was Defined by Julian Treasure A2Document2 pagesListening Was Defined by Julian Treasure A2kim olimbaNo ratings yet
- Gas Leakage Detection Using Arm7 and ZigbeeDocument18 pagesGas Leakage Detection Using Arm7 and ZigbeevinjamurisivaNo ratings yet