You might also like
- Keywords: Farmer, Pesticide, Respiratory DisorderDocument18 pagesKeywords: Farmer, Pesticide, Respiratory Disorderdyan ayu puspariniNo ratings yet
- Deeble Institue Issues Brief No 19 1Document15 pagesDeeble Institue Issues Brief No 19 1dyan ayu puspariniNo ratings yet
- Hypertension and Herbal Plant For Its Treatment: A ReviewDocument1 pageHypertension and Herbal Plant For Its Treatment: A Reviewdyan ayu puspariniNo ratings yet
- Al., 2011) - It Is Thus Expedient To Prepare The Public Health Nursing Work-Force WithinDocument9 pagesAl., 2011) - It Is Thus Expedient To Prepare The Public Health Nursing Work-Force Withindyan ayu puspariniNo ratings yet
- 9.2: Searching The Literature: Resource Web Site CommentDocument6 pages9.2: Searching The Literature: Resource Web Site Commentdyan ayu puspariniNo ratings yet
- WHO - PneumoniaDocument4 pagesWHO - Pneumoniadyan ayu puspariniNo ratings yet
- Antioxidants and Chlorophyll in Cassava Leaves at Three Plant AgesDocument7 pagesAntioxidants and Chlorophyll in Cassava Leaves at Three Plant Agesdyan ayu puspariniNo ratings yet
- Anti-Inflammatory, Analgesic and Anti - Pyretic Activity of Cassava Leaves ExtractDocument4 pagesAnti-Inflammatory, Analgesic and Anti - Pyretic Activity of Cassava Leaves Extractdyan ayu puspariniNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Contribution of Tourism Industry in Indian Economy: An AnalysisDocument8 pagesContribution of Tourism Industry in Indian Economy: An AnalysisHarsh GuptaNo ratings yet
- Mastery Problem (L04, 5, 6), 27: 2,500 500 0 200 100 1,300 1,500 (Expense) 2,000 0 200 100 1,300 1,000Document2 pagesMastery Problem (L04, 5, 6), 27: 2,500 500 0 200 100 1,300 1,500 (Expense) 2,000 0 200 100 1,300 1,000Paulina OlivaresNo ratings yet
- COM379 Essay 7Document5 pagesCOM379 Essay 7Ali RungeNo ratings yet
- Automatic Site PositioningDocument1 pageAutomatic Site PositioningDenmark Wilson0% (1)
- Summarydoc Module 2 LJGWDocument14 pagesSummarydoc Module 2 LJGWKashish ChhabraNo ratings yet
- S F R S (I) 1 - 2 1: Accounting For The Effects of Changes in Foreign Currency Exchange RatesDocument40 pagesS F R S (I) 1 - 2 1: Accounting For The Effects of Changes in Foreign Currency Exchange RatesRilo WiloNo ratings yet
- Ch13 (Man)Document44 pagesCh13 (Man)kevin echiverriNo ratings yet
- 35 Childrens BooksDocument4 pages35 Childrens Booksapi-710628938No ratings yet
- Roman-Macedonian Wars Part 1Document2 pagesRoman-Macedonian Wars Part 1Alxthgr8No ratings yet
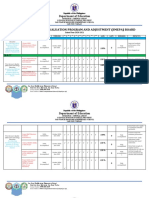
- SJDM Es Smepa Board 2020-2021Document5 pagesSJDM Es Smepa Board 2020-2021Loreto Capitli MoralesNo ratings yet
- Tax Invoice/Bill of Supply/Cash Memo: (Original For Recipient)Document1 pageTax Invoice/Bill of Supply/Cash Memo: (Original For Recipient)Raj SakariaNo ratings yet
- Vasco Menu - Monthly Festive Dinner 2023Document4 pagesVasco Menu - Monthly Festive Dinner 2023Heamalatha Raja ManickamNo ratings yet
- (Digest) Marcos II V CADocument7 pages(Digest) Marcos II V CAGuiller C. MagsumbolNo ratings yet
- HirarchaddonDocument5 pagesHirarchaddonawe_emNo ratings yet
- Environmental Change and ComplexityDocument7 pagesEnvironmental Change and ComplexityIffah Nadzirah100% (2)
- Descriptive Text TaskDocument12 pagesDescriptive Text TaskM Rhaka FirdausNo ratings yet
- The Officers of Bardwell Company Are Reviewing The ProfitabilityDocument1 pageThe Officers of Bardwell Company Are Reviewing The ProfitabilityAmit PandeyNo ratings yet
- Gyges RingDocument1 pageGyges RingCYRINE HALILINo ratings yet
- Creating A Carwash Business PlanDocument7 pagesCreating A Carwash Business PlanChai Yeng LerNo ratings yet
- Legal Acctng CasesDocument108 pagesLegal Acctng CasesJerry Barad SarioNo ratings yet
- Power of The High Courts To Transfer CasesDocument2 pagesPower of The High Courts To Transfer CasesShweta ChauhanNo ratings yet
- Q2 - Week 7 8Document4 pagesQ2 - Week 7 8Winston MurphyNo ratings yet
- UNCLOS - Salient Features, Objectives, Maritime Zones, Passages and DutiesDocument14 pagesUNCLOS - Salient Features, Objectives, Maritime Zones, Passages and DutiesGiorgi KandelakiNo ratings yet
- Classification and Use of LandDocument5 pagesClassification and Use of LandShereenNo ratings yet
- Name: Nitesh Bagla Enrollment No: 19Bsp1776 IBS Campus: Kolkata Mobile No: 9681759023 E-Mail Id: SIP Proposal I. SIP ProposedDocument3 pagesName: Nitesh Bagla Enrollment No: 19Bsp1776 IBS Campus: Kolkata Mobile No: 9681759023 E-Mail Id: SIP Proposal I. SIP ProposedNitesh BaglaNo ratings yet
- Universalism and Cultural Relativism in Social Work EthicsDocument16 pagesUniversalism and Cultural Relativism in Social Work EthicsEdu ArdoNo ratings yet
- Guilatco Vs City of Dagupan Case DigestDocument1 pageGuilatco Vs City of Dagupan Case DigestYrna Caña100% (1)
- My Father's Goes To Cour 12-2Document34 pagesMy Father's Goes To Cour 12-2Marlene Rochelle Joy ViernesNo ratings yet
- 137684-1980-Serrano v. Central Bank of The PhilippinesDocument5 pages137684-1980-Serrano v. Central Bank of The Philippinespkdg1995No ratings yet
- LWB Manual PDFDocument1 pageLWB Manual PDFKhalid ZgheirNo ratings yet