Professional Documents
Culture Documents
Caries Risk Assessment PDF
Uploaded by
Hanif Zhafran Alif LaodeOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Caries Risk Assessment PDF
Uploaded by
Hanif Zhafran Alif LaodeCopyright:
Available Formats
Pediatric Dentistry
CDE
2 HOURS
CREDIT
Caries risk assessment, prevention, and
management in pediatric dental care
Francisco Ramos-Gomez, DDS, MS, MPH Yasmi O. Crystal, DMD
n n Man Wai Ng, DDS, MPH
Norman Tinanoff, DDS, MS John D. Featherstone, MSc, PhD
n
The recent increase in the prevalence of dental caries among young the dental home and a simple six-step protocol to conduct an
children has highlighted the need for a new approach to prevent effective and comprehensive infant oral care visit. Age-specific
caries in children at a younger age. New disease prevention anticipatory guidance recommendationsincluding early parental
management models call for children to have their first visit to education, timely intervention, and/or referralhave been
the dentist at age 1 or when their first tooth erupts. This article included for counseling parents during early childhood dental visits.
addresses early childhood caries risk assessment, prevention, and Received: March 30, 2010
management strategies in young children using the concept of Accepted: June 15, 2010
T
he general dentist is in the age groups, where caries rates remain Establishment of a
unique position of establishing unchanged, the caries rate among dental home
a dental care program for preg- preschoolers has increased to 28%.7,8 Signs of ECC can be detected soon
nant women, which is considered It is well-documented that caries after the eruption of the first tooth.
the first step toward disease preven- is a transmissible infectious disease Its progression is entirely prevent-
tion for infants and toddlers. in which pathogenic risk factors able, provided that risk indicators
prevail over protective factors, are identified and preventive oral
Background producing demineralization of tooth health practices are implemented
Dental caries remains the most prev- structure. If the disease is allowed at a young age.14 For this reason,
alent chronic childhood disease in to progress, surface cavitation and the AGD, the ADA, the American
the U.S., five times more common dental tissue destruction will result. Academy of Pediatric Dentistry, and
than asthma and seven times more Mutans streptococci (MS) is con- the American Academy of Pediatrics
common than hay fever.1-3 This sidered one of the most important all have recommended that children
disease, known as early childhood pathogens in the cariogenic process should see a dentist by age 1 (or
caries (ECC) (formerly termed because of its ability to stick to when the first tooth erupts) and
nursing bottle caries or baby bottle smooth tooth surfaces and produce that a dental home be established
tooth decay), is currently defined as copious amounts of acid. It is rec- as soon as possible.4,15,16 The dental
the presence of one or more decayed ognized that these micro-organisms home is defined as the ongoing
(that is, cavitated or noncavitated can be transmitted from caregiver relationship between the dentist and
lesions), missing (due to caries), or to child through close contact with the patientincluding all aspects
filled surfaces in any primary tooth or through the exchange of saliva of oral health caredelivered in a
in a child age 6 or younger.4 Among (vertical transmission)for example, comprehensive, continuously acces-
children under the age of 3, any sign through kissing on the mouth, sible, coordinated, family-centered
of smooth-surface caries is indica- sharing utensils or cups, and so way.16 Establishment of a dental
tive of severe early childhood caries forth. Caregivers with high levels of home (including referral to dental
(S-ECC).4 ECC is prevalent among pathogenic bacteria in their mouths specialists when appropriate) should
young children, particularly in can communicate these bacteria into begin by the time the child is 12
underserved populations and racial/ a childs mouth even before the erup- months old.16
ethnic minorities.5 Approximately tion of the first tooth. It has been A dental home should be estab-
75% of ECC is found in approxi- shown that infants with high levels of lished so that children can make
mately 8% of children between the MS or those with early colonization regular dental visits that include
ages of 2 and 5.6 Compared to other are more likely to develop ECC.9-13 caries risk assessment, individualized
www.agd.org General Dentistry November/December 2010 505
Pediatric Dentistry Caries risk assessment, prevention, and management in pediatric dental care
The benefits of prevention, diag-
nosis, and treatment of oral diseases
(including the use of radiographs
and local anesthetics) during preg-
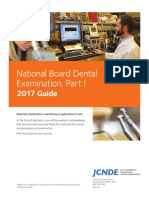
Pathological factors nancy exceed the risks inherent in
Acid-producing bacteria treatment or those associated with
Frequent eating/drinking of not providing care. Improving the
Protective factors
fermentable carbohydrates oral health of expectant mothers by
Subnormal saliva flow and Saliva flow and components
reducing their pathogenic bacteria
function Fluoride: Remineralization
with calcium and phosphate levels will postpone the childs
Antibacterials: Chlorhexidine, acquisition of oral bacteria and may
xylitol, and others delay the development of ECC.23
Initial infant oral care visit
Infants and parents will benefit
from an early infant oral health visit
and the establishment of a dental
home. Explaining exactly what to
expect during this visit may allay
Caries No caries parental fears and concerns. Parents
should be warned that children
Fig. 1. An illustration of the caries balance concept. might cry during the visit, just as
they would when they are hungry,
tired, or placed in a new situation.
Understanding the benefits of this
preventive visit will help parents
preventive strategies, and anticipa- Perinatal oral health cope, even if their child cries and is
tory guidance.17 Periodic supervision Dentists have come to recognize uncooperative.
of care intervals (also known as the critical role that a mother An infant oral care examination
periodicity) should be determined plays in ensuring her childs oral and caries risk assessment follows
based on the disease risk for each health. However, women often do a simple six-step protocol, as
individual patient.16 not receive oral health care and described below.
Pediatricians, family practitioners, education in a timely manner.19
and other medical providers see Many women do not know that Caries risk assessment
children frequently during infancy they should seek dental care during An individualized risk assessment of
and early childhood. These practi- their pregnancy, while many others an infant or toddler will help both
tioners are ideally suited to screen who do know this are often unable health care providers and parents/
young children for caries risk and to find a dentist who is willing to caregivers identify and understand
refer these patients for dental care. provide it.20 Because new mothers the factors associated with ECC, so
If physicians are to refer children for are more likely to be receptive to that a cooperative and proactive pre-
their first dental visit at age 1, the ideas that would improve their ventive care plan can be developed.
dental community must be willing offsprings oral health, dental and The specific information gained
and prepared to accept infants and obstetric providers have a prime from a systematic assessment of
pregnant women as patients. Since opportunity to educate mothers caries risk guides the dentist in the
general dentists comprise 80% about the changes that could affect decision-making process to establish
of practicing dentists and see the their children.21 It is important for treatment and preventive protocols
majority of children seeking dental general dentists to provide expect- for children with oral disease and
care, it is important for these den- ant mothers with comprehensive for those deemed to be at risk.
tists to embrace the concepts of the dental care, as recent studies have To achieve the best management
dental home, infant oral health, and shown that it is safe to provide care and outcomes for good oral health,
perinatal health.18 at any point during pregnancy.22-24 the caries risk assessment should be
506 November/December 2010 General Dentistry www.agd.org
done as early as possiblepreferably
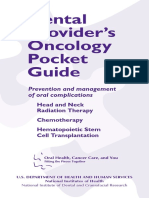
before the onset of disease. Caries Childs name: ________________________________________________________
risk assessment and subsequent
management of the disease in High risk Moderate Protective
Biological factors factors risk factors factors
children is crucial due to the known
fact that caries in the primary denti- Mother/primary caregiver has active caries Yes
tion is a strong predictor of caries in Parent/caregiver has low socioeconomic status Yes
the permanent dentition.25,26 Child has more than three snacks or beverages Yes
The caries balance concept states containing sugar per day between meals
that the progression or reversal Child is put to bed with a bottle containing Yes
of dental caries is determined by natural or added sugar
the balance between pathologi- Child has special health care needs Yes
cal factors and protective factors Child is a recent immigrant Yes
(Fig. 1).27-29 These risk factors are
Protective factors
determined from interviews with
Child receives fluoridated drinking water or Yes
the parent(s) and a clinical assess-
fluoride supplements
ment. The caries risk assessment
Childs teeth are brushed daily with fluoridated Yes
form in Figure 2 provides an easy
toothpaste
way to compile and keep a record
Child receives topical fluoride from health Yes
of the information that will aid
professional
the dentist in determining the
Child has dental home/regular dental care Yes
infant/childs caries risk. This form
is broken down into three major Clinical findings
categories: biological risk factors, Child has more than one decayed, missing, or Yes
protective factors, and disease indi- filled tooth surface (DMFS)
cators from a clinical examination. Child has active white spot lesions or enamel Yes
Biological risk factors are defects
obtained from the caretaker Child has elevated mutans streptococci Yes
interview and include biological or Child has plaque on teeth Yes
lifestyle factors that contribute to Modified from: Ramos-Gomez F, Crall J, Slayton R, Featherstone JD. Caries risk assessment appropriate
the development or progression of for the age one visit. J Calif Dent Assoc 2007;35(10):687-702; and ADA Caries Risk Assessment Forms.
caries. These risk factors include
a mother with active decay or Circling those conditions that apply to a specific patient helps the practitioner and parent
recently placed dental restorations, understand the factors that contribute to or protect against caries. Risk assessment
a family with a low socioeconomic categorization of low, moderate, or high is based on a preponderance of factors. However,
status, a caregiver with low health clinical judgment may justify the use of one factor in determining overall risk, for instance,
frequent exposure to sugar-containing snacks or beverages, or more than one DMFS.
literacy, and a child who frequently
intakes fermentable carbohydrates
or sweetened drinks and/or sleeps Overall assessment of the childs dental caries risk:
with a bottle or sippy cup contain- High Moderate Low
ing milk or juice.
Protective factors are also Self-management goals:
obtained during the interview. 1_________________________________ 2________________________________
These are biological and/or
therapeutic factors, measures, and Practitioner signature: ________________________________________________
behaviors that, when used consis- Date: _______________________________________________________________
tently, could reduce a childs risk for
ECC. These factors include optimal
exposure to fluoride and access to
regular dental care (for example, Fig. 2. A sample caries risk assessment form for children from ages 15. ( Copyright 2010-2011
the presence of a dental home). by the American Academy of Pediatric Dentistry. Reprinted with permission.)
www.agd.org General Dentistry November/December 2010 507
Pediatric Dentistry Caries risk assessment, prevention, and management in pediatric dental care
Table 1. CAMBRA dental caries treatment protocol guidelines for children up to age 2.
Diagnostic
Periodic
Risk oral Saliva
category examinations Radiographs test Fluoride
Low Annual Posterior bitewings at 1224 month intervals if Optional In office: no; Home: brush twice each day with a smear
proximal surfaces cannot be examined visually or baseline of fluoride toothpaste
with a probe
Moderate Every six Posterior bitewings at 612 month intervals if Recom- In office: FV at initial visit and recalls; Home: brush
months proximal surfaces cannot be examined visually or mended twice each day with a smear of fluoride toothpaste;
with a probe Caregiver: OTC sodium fluoride treatment rinses
Moderate; Every three Posterior bitewings at 612 month intervals if Required In office: FV at initial visit and recalls; Home: brush
non- to six months proximal surfaces cannot be examined visually or twice a day with a smear of fluoride toothpaste
compliant with a probe combined with a smear of 900 ppm calcium phosphate
paste, leave on at bedtime; Caregiver: OTC sodium
fluoride treatment rinses
High Every three Anterior (No. 2 occlusal film) and posterior Required In office: FV at initial visit and recalls; Home: brush
months bitewings at 612 month intervals if proximal twice a day with a smear of fluoride toothpaste
surfaces cannot be examined visually or with a combined with a smear of 900 ppm calcium phosphate
probe paste, leave on at bedtime; Caregiver: OTC sodium
fluoride treatment rinses
High; non- Every one Anterior (No. 2 occlusal film) and posterior Required In office: FV at initial visit and recalls; Home: brush
compliant to three bitewings at 612 month intervals if proximal twice a day with a smear of fluoride toothpaste
months surfaces cannot be examined visually or with a combined with a smear of 900 ppm calcium phosphate
probe paste, leave on at bedtime; Caregiver: OTC sodium
fluoride treatment rinses
Extreme Every one Anterior (No. 2 occlusal film) and posterior Required In office: FV at initial visit and recalls; Home: brush
to three bitewings at 612 month intervals if proximal twice a day with a smear of fluoride toothpaste
months surfaces cannot be examined visually or with a combined with a smear of 900 ppm calcium phosphate
probe paste, leave on at bedtime; Caregiver: OTC sodium
fluoride treatment rinses
Disease indicators are findings,
obtained during the clinical
examination of the child, that
are proven to have a strong
correlation to the presence of the
disease. These include cavitated
carious lesions and white spot
lesions/decalcifications, recent
restorations, presence of plaque,
gingival bleeding (an indicator of
heavy plaque), and dry mouth.
A risk assessment categoriza-
tion of low, moderate, or high is
based on a preponderance of the
Fig. 3. An example of the knee-to-knee position. factors circled on the caries risk
508 November/December 2010 General Dentistry www.agd.org
Preventive intervention Restoration
Anticipatory Self-
guidance management White spots/
Xylitol Sealants Antibacterials /counseling goals precavitated lesions Existing lesions
Not required No No Yes No n/a n/a
Child: xylitol wipes; Fluoride-releasing No Yes No Treat with fluoride n/a
Caregiver: two sticks sealants recom- products as
of gum or two mints mended on deep indicated to promote
four times a day pits and fissures remineralization
Child: xylitol wipes; Fluoride-releasing Recommend Yes Yes Treat with fluoride n/a
Caregiver: two sticks sealants recom- for caregiver products as
of gum or two mints mended on deep indicated to promote
four times a day pits and fissures remineralization
Child: xylitol wipes; Fluoride-releasing Recommend Yes Yes Treat with fluoride Intermediate therapeutic
Caregiver: two sticks sealants recom- for caregiver products as restoration (ITR) or
of gum or two mints mended on deep indicated to promote conventional restorative
four times a day pits and fissures remineralization treatment as patient
cooperation and family
circumstances allow
Child: xylitol wipes; Fluoride-releasing Recommend Yes Yes Treat with fluoride ITR or conventional
Caregiver: two sticks sealants recom- for caregiver products as restorative treatment as
of gum or two mints mended on deep indicated to promote patient cooperation and
four times a day pits and fissures remineralization family circumstances allow
Child: xylitol wipes; Fluoride-releasing Recommend Yes Yes Treat with fluoride ITR or conventional
Caregiver: two sticks sealants recom- for caregiver products as restorative treatment as
of gum or two mints mended on deep indicated to promote patient cooperation and
four times a day pits and fissures remineralization family circumstances allow
assessment form. These specific findings and receive hygiene for the child. The clinician should
patient conditions will help both instructions while gently helping explain what will happen prior
the practitioner and the parent(s) to stabilize the child during the to starting the examination and
understand the factors that con- examination. In general, the knee- anticipate that young children
tribute to or protect the patient to-knee position should be used might cry, which is developmen-
from caries. for children between the ages of 6 tally appropriate behavior.
months and 3 years, or up to age 5
Proper positioning for children with special health care Toothbrush prophylaxis
Proper positioning of the child is needs. Children over the age of 3 For most young children, a
critical to conducting an effective may be able to sit forward on their toothbrush prophylaxis is efficient
and efficient clinical examination. caregivers lap or sit alone in a chair. for removing plaque. It is also
Knee-to-knee positioning (Fig. 3) Examiners and caregivers need non-threatening to young children
allows the child to see the parent to work together to ensure that and serves to demonstrate the
throughout the examination, while the transition from the interview proper technique of brushing to the
the parent can directly observe to the examination runs smoothly caregiver.30,31
www.agd.org General Dentistry November/December 2010 509
Pediatric Dentistry Caries risk assessment, prevention, and management in pediatric dental care
Table 2. CAMBRA dental caries treatment protocol for children from ages 36.
Diagnostic
Periodic
Risk oral Saliva
category examinations Radiographs test Fluoride
Low Annual Posterior bitewings at 1224 month intervals if Optional In office: no; Home: brush twice a day with a
proximal surfaces cannot be examined visually baseline pea-sized amount of fluoride toothpaste
or with a probe
Moderate Every six Posterior bitewings at 612 month intervals if Recom- In office: FV at initial visit and recalls; Home:
months proximal surfaces cannot be examined visually mended brush twice a day with a pea-sized amount of
or with a probe fluoride toothpaste; Caregiver: OTC sodium fluoride
treatment rinses
Moderate; Every three Posterior bitewings at 612 month intervals if Required In office: FV at initial visit and recalls; Home: brush
non- to six months proximal surfaces cannot be examined visually twice a day with a pea-size of fluoride toothpaste
compliant or with a probe combined with a pea-size of 900 ppm calcium
phosphate paste, leave on at bedtime; Caregiver:
OTC sodium fluoride treatment rinses
High Every three Anterior (No. 2 occlusal film) and posterior Required In office: FV at initial visit and recalls; Home: brush
months bitewings at 612 month intervals if proximal twice a day with a pea-size of fluoride toothpaste
surfaces cannot be examined visually or with combined with a pea-size of 900 ppm calcium
a probe phosphate paste, leave on at bedtime; Caregiver:
OTC sodium fluoride treatment rinses
High; non- Every one to Anterior (No. 2 occlusal film) and posterior Required In office: FV at initial visit and recalls; Home: brush
compliant three months bitewings at 612 month intervals if proximal twice a day with a pea-size of fluoride toothpaste
surfaces cannot be examined visually or with combined with a pea-size of 900 ppm calcium
a probe phosphate paste, leave on at bedtime; Caregiver:
OTC sodium fluoride treatment rinses
Extreme Every one Anterior (No. 2 occlusal film) and posterior Required In office: FV at initial visit and recalls; Home: brush
to three bitewings at 612 month intervals if proximal twice a day with a pea-size of fluoride toothpaste
months surfaces cannot be examined visually or with combined with a pea-size of 900 ppm calcium
a probe phosphate paste, leave on at bedtime; Caregiver:
OTC sodium fluoride treatment rinses
For this step, the examiner A pea-sized amount of toothpaste the child at each step for his or her
retracts the childs lips and cheeks is recommended for children cooperation and/or good behavior.
and demonstrates brushing along between the ages of 2 and 6, while a If the child is able to cooperate, the
the gingival margins. The spongy smear is appropriate for children examiner should also inspect the
handle of an age-appropriate under the age of 2.34 soft tissues, hard tissues, and occlu-
toothbrush can be used to prop sion at this time.
open the childs mouth. During Clinical examination Data from the clinical examina-
this Tell-Show-Do encounter, During this examination, the exam- tion should be combined with
caregivers should be encouraged iner counts the childs teeth aloud, data from the caregiver interview
to brush both their own teeth and using the toothbrush handle to to determine the childs overall
the childs at least twice a day, prop open the mouth if necessary. caries risk and formulate an indi-
especially before bedtime. Fluoride Many providers make a game of this vidualized treatment plan. Visible
toothpaste is one of the most effec- task, singing songs, engaging the plaque and its locations should
tive tools for caries prevention and childs attention, and, if all else fails, be documented, as should white
it is safe for children to use as soon distracting the child with a brightly spot lesions, brown spots (which
as the first tooth erupts.32,33 colored toothbrush or toy. Praise may indicate caries on the occlusal
510 November/December 2010 General Dentistry www.agd.org
Preventive intervention Restoration
Anticipatory Self- White spot/
guidance/ management precavitated
Xylitol Sealants Antibacterials counseling goals lesions Existing Lesions
Not required No No Yes No n/a n/a
Child: xylitol wipes/products Fluoride-releas- No Yes No Treat with fluoride n/a
to substitute for sweet treats ing sealants products as indi-
or when unable to brush; recommended cated to promote
Caregiver: two sticks of gum on deep pits and remineralization
or two mints four times a day fissures
Child: xylitol wipes/products Fluoride-releas- Recommend Yes Yes Treat with fluoride n/a
to substitute for sweet treats ing sealants for caregiver products as indi-
or when unable to brush; recommended cated to promote
Caregiver: two sticks of gum on deep pits and remineralization
or two mints four times a day fissures
Child: xylitol wipes/products Fluoride-releas- Recommend Yes Yes Treat with fluoride ITR or conventional
to substitute for sweet treats ing sealants for caregiver products as indi- restorative treatment
or when unable to brush; recommended cated to promote as patient coop-
Caregiver: two sticks of gum on deep pits and remineralization eration and family
or two mints four times a day fissures circumstances allow
Child: xylitol wipes/products Fluoride-releas- Recommend Yes Yes Treat with fluoride ITR or conventional
to substitute for sweet treats ing sealants for caregiver products as indi- restorative treatment
or when unable to brush; recommended cated to promote as patient coop-
Caregiver: two sticks of gum on deep pits and remineralization eration and family
or two mints four times a day fissures circumstances allow
Child: xylitol wipes/products Fluoride-releas- Recommend Yes Yes Treat with fluoride ITR or conventional
to substitute for sweet treats ing sealants for caregiver products as indi- restorative treatment
or when unable to brush; recommended cated to promote as patient coop-
Caregiver: two sticks of gum on deep pits and remineralization eration and family
or two mints four times a day fissures circumstances allow
surface), tooth defects, deep pits/fis- with fluoridated water. The provider risk assessment form, the practitio-
sures, tooth anomalies, missing and should reiterate the cumulative ner can evaluate and determine the
decayed teeth, existing and defec- benefit of FV, even if it has been childs risk for developing carious
tive restorations, gingivitis or other mentioned earlier in the visit. After lesions. The practitioner should
soft tissue abnormalities, occlusion, application, the child should be record all Yes answers to each
and indications of trauma. limited to a soft diet (that is, no question within the three areas
crunchy or chewy foods) for the of risk assessment and record any
Fluoride treatment remainder of the day; in addition, No answers to a protective factor
The ADA recommends that for the varnish to be effective, the under the High Risk column.
children categorized as high caries parent/caregiver should not brush A No response to a protective
risk receive a full-mouth topical the childs teeth until the next day. factor is equal to a high risk factor.
fluoride varnish (FV) application High risk factors can be mitigated
every three months.35 Children Assignment of risk, anticipatory by affirmative protective factors,
with a moderate caries risk should guidance, and counseling which help to determine if a child
receive FV every six months, even Once all of the data have been is at moderate or even low risk for
if the child lives in a community gathered and recorded in the caries caries development.
www.agd.org General Dentistry November/December 2010 511
Pediatric Dentistry Caries risk assessment, prevention, and management in pediatric dental care
Table 3. Age-specific anticipatory guidance.
Prenatal Birth to age 1 Ages 23 Ages 36
Take-home Baby teeth are important! Baby teeth are important! Baby teeth are important! Baby teeth are important!
message for Parents/caregivers oral health Parents/caregivers oral health Parents/caregivers oral Parents/caregivers oral
caregivers affects the babys oral health. affects the babys oral health. health affects the babys health affects the childs
oral health. oral health.
Parents/caregivers should Parents/caregivers should obtain
obtain regular dental regular dental check-ups and get Parents/caregivers should Parents/caregivers should
check-ups and get treatment if treatment if necessary. obtain regular dental check- obtain regular dental check-
necessary. ups and get treatment if ups and get treatment if
Parents/caregivers should avoid
necessary. necessary.
Schedule childs first dental sharing with their child things that
appointment by age 1. have been in their mouths. Parents/caregivers should Parents/caregivers should
avoid sharing with their avoid sharing with their
Use of fluorides, including Schedule childs first dental
child things that have been child things that have been
brushing the teeth with a appointment by age 1.
in their mouths. in their mouths.
fluoride toothpaste, is the most Prevention is less costly than
effective way to prevent tooth Prevention is less costly Prevention is less costly
treatment.
decay than treatment. than treatment.
Use of fluorides, including brushing
Use of fluorides, including Use of fluorides, including
the teeth with a fluoride toothpaste,
brushing the teeth with brushing the teeth with
is the most effective way to prevent
a fluoride toothpaste, is a fluoride toothpaste, is
tooth decay.
the most effective way to the most effective way to
prevent tooth decay. prevent tooth decay.
Oral health Encourage parents/caregivers Encourage parents/caregivers to Encourage parents/caregiv- Encourage parents/caregiv-
and hygiene to obtain dental check-ups maintain good oral health and get ers to maintain good oral ers to maintain good oral
and, if necessary, treatment treatment, if necessary, to reduce health and get treatment, health and get treatment,
before birth of the baby to the spread of bacteria that can cause if necessary, to reduce the if necessary, to reduce the
reduce cavity-causing bacteria tooth decay. spread of bacteria that can spread of bacteria that can
that can be passed to the baby. cause tooth decay. cause tooth decay.
Encourage parents/caregivers to
Encourage parents/caregivers avoid sharing with their child things Encourage parents/caregiv- Encourage parents/caregiv-
to brush teeth with fluoride that have been in their mouths. ers to avoid sharing with ers to avoid sharing with
toothpaste. their child things that have their child things that have
Encourage parents/caregivers to
been in their mouths. been in their mouths.
become familiar with the normal
appearance of the childs gums. Review parents/caregivers Discuss the continued
role in brushing toddlers responsibility of parents/
Emphasize using a washcloth or
teeth. caregivers to help children
toothbrush to clean teeth and gums
under 8 to brush their teeth.
after the eruption of the first tooth. Discuss brush and
toothpaste selection. Encourage parents/caregiv-
Encourage parents/caregivers to
ers to consider dental
check front and back teeth for white, Problem-solve oral hygiene
sealants for primary and
brown, or black spots (signs of issues.
permanent first molars
cavities).
Oral Describe primary tooth Discuss primary tooth eruption Emphasize importance of Emphasize importance of
development eruption patterns (first tooth patterns. baby teeth for chewing, baby teeth for chewing,
usually erupts between 6 and speaking, jaw development, speaking, jaw development,
Emphasize importance of baby
10 months of age). and self-esteem. and self-esteem.
teeth for chewing, speaking, jaw
Emphasize importance of baby development, and self-esteem. Discuss teething and ways
teeth for chewing, speaking, to soothe sore gums, such
Discuss teething and ways to soothe
jaw development, and as chewing on teething
sore gums, such as chewing on
self-esteem. rings and washcloths.
teething rings and washcloths.
512 November/December 2010 General Dentistry www.agd.org
Prenatal Birth to age 1 Ages 23 Ages 36
Fluoride Evaluate fluoride status of Evaluate fluoride status of residential Re-evaluate fluoride status Re-evaluate fluoride status
adequacy residential water supply water supply. of residential water supply. of residential water supply.
Review topical and systemic Review topical and systemic sources Review topical and systemic Review topical and systemic
sources of fluoride. of fluoride. sources of fluoride. sources of fluoride.
Encourage mother to drink Encourage drinking fluoridated tap Encourage drinking Review need for topical or
fluoridated tap water. water. fluoridated tap water. other fluorides.
Consider topical needs (e.g., Review need for topical
toothpaste, fluoride varnish). fluorides.
Oral habits Encourage mother to stop Encourage breastfeeding. Remind mother that Discuss consequences of
smoking removing child from breast digit sucking and prolonged
Advise mother that removing child
after feeding and wiping non-nutritive sucking
from breast after feeding and wiping
babys gums/teeth with a (e.g., pacifier) and begin
babys gums/teeth with a damp
damp washcloth reduces professional intervention if
washcloth reduces the risk of ECC.
the risk of ECC. necessary.
Review pacifier safety.
Begin weaning of
non-nutritive sucking habits
at age 2.
Diet and Emphasize eating a healthy Remind parents/caregivers never to Remind parents/caregivers Review and encourage a
nutrition diet and limiting the number put the baby to bed with a bottle never to put the baby to healthy diet.
of exposures to sugar snacks containing anything other than water bed with a bottle or to Remind parents/caregivers
and drinks. or to allow feeding at will. allow feeding at will. about limiting the frequency
Emphasize that it is the Emphasize that it is the frequency of Discuss a healthy diet and of exposures to sugar.
frequency of exposures, not exposures, not the amount of sugar, oral health. Review snacking choices.
the amount of sugar, that that affects susceptibility to caries.Emphasize that it is the
affects susceptibility to caries. Emphasize that the child
Encourage weaning from bottle to frequency of exposures, should be completely
Encourage breastfeeding. cup by age 1. not the amount of sugar, weaned from the bottle
Remind parents/caregivers Encourage diluting juices with water. that affects susceptibility and should be drinking
to caries.
never to put the baby to exclusively from a cup.
bed with a bottle containing Review snack choices and
anything other than water or encourage healthy snacks.
to allow feeding at will.
Injury Encourage childproofing of Review childproofing of home, Review childproofing of Emphasize the use of a
prevention home, including electrical cord including electrical cord safety and home, including electrical properly secured car seat.
safety and poison control. poison control. cord safety and poison Encourage safety in play
control.
Emphasize the use of a Emphasize the use of a properly activities, including helmets
properly secured car seat. secured car seat. Emphasize the use of a when riding bikes and
properly secured car seat. mouthguards when playing
Encourage caregivers to keep Encourage caregivers to keep
sports.
emergency numbers handy. emergency numbers handy. Emphasize the use of a
helmet when child is riding Remind caregivers to keep
a tricycle/bicycle or is in the emergency numbers handy.
seat of an adult bike.
Remind caregivers to keep
emergency numbers handy.
www.agd.org General Dentistry November/December 2010 513
Pediatric Dentistry Caries risk assessment, prevention, and management in pediatric dental care
Tooth decay is caused by certain types of bacteria (bugs) that live in your mouth. When they stick For example, children who
to the film on your teeth (also called dental plaque), they can cause damage. The bacteria feed frequently eat snacks or drink juice
on what you eat, especially sugars (including fruit sugars) and cooked starches (bread, potatoes,
may be at only moderate risk if they
rice, pasta, etc.). Within approximately five minutes after you eat or drink, the bacteria begin
making acids as they digest your food. These acids can break into the outer surface of the tooth live in a community that has fluori-
and melt away some of the minerals. Your saliva can balance the acid attacks as long as they dated water and if they brush twice
dont happen very often. However, if: 1) your mouth is dry, 2) you have a lot of these bacteria, or a day with a fluoride toothpaste.
3) you snack frequently, then the acid causes the loss of tooth minerals. This is the start of tooth However, some factors are prepon-
decay and leads to cavities.
derant, and a Yes response to the
Methods of controlling tooth decay Bacteria
biological factor Mother/primary
Diet caregiver has active caries or to the
Reducing the amount of sugary and starchy clinical findings Child has more
foods, snacks, and drinks you consume can
than one decayed, missing, or filled
help to reduce tooth decay. This doesnt
mean that you can never eat these types of
Sugar tooth surface (dmfs) or Child has
foods, just that you should limit the number active white spot lesions or enamel
of times you eat them between main meals. defects immediately places the
A good rule is three meals per day and no Acid
child at high or extreme high risk.
more than three snacks per day.
When the risk factors outweigh
Fluorides the protective factors, there is an
Fluorides help to make teeth stronger, to protect against tooth decay, and to heal tooth decay if it increased likelihood for the devel-
has not gone too far. Fluorides are available from a variety of sources, such as drinking water and
toothpastes and rinses you can buy at the supermarket or drug store. They may also be prescribed
opment of caries, which places the
by your dentist or applied in the dental office. The daily use of fluoride is very important to help child in a high risk category. When
protect against the acid attacks. protective factors prevail and risk
Plaque removal factors are controlled, the child
Plaque is a yellowish film that sticks to the surface of teeth. Brushing your teeth removes plaque can be considered low risk. Most
and should be done twice every day. Bacteria live in plaque, so removing the plaque from your importantly, though, the clinicians
teeth on a daily basis helps to control tooth decay. Plaque is very sticky and may be hard to experience and expertise is a vital
remove from between your teeth and from the grooves on the biting surfaces of your back teeth.
component for determining a
If your child has an orthodontic retainer, be sure to remove it before brushing your childs teeth.
Brush all surfaces of the retainer as well. childs ultimate risk, which serves
as the basis for an individualized
Saliva
Saliva is important for healthy teeth. It balances acids and provides other ingredients that protect treatment plan for each infant
the teeth. If you cannot brush after a meal or snack, you can chew sugar-free gum. This will and caregiver. An approach that
stimulate the flow of saliva to help reduce the effect of acids. Sugar-free candy or mints can also considers expected parental compli-
be used, but some of them contain acids themselves. Acids in sugar-free candy will not cause ance to recommended treatment
tooth decay, but they can slowly dissolve the tooth surface over time (a process called erosion ).
protocols is essential for children at
Some sugar-free gums are made to help fight tooth decay, while some gums contain baking soda,
which neutralizes the acids produced by the bacteria in plaque. Gum that contains xylitol as moderate or high caries risk.
its first listed ingredient is the gum of choice. This type of gum has been shown to protect The treatment protocol guide-
against tooth decay and to reduce the number of bacteria that cause decay. lines presented in this article
Antibacterial mouthrinses outline care paths for children
Rinses that your dentist can prescribe are able to reduce the number of bacteria that cause tooth with moderate or high risk as well
decay and can be useful in patients at high risk for tooth decay. These rinses are recommended as guidelines for a child who has
only for children who can rinse and spit. non-compliant parents and who
Sealants
is at moderate or high risk. Table
Sealants are plastic coatings brushed onto the biting surfaces of back teeth to protect the deep 1 lists caries management by risk
grooves from decay. In some people, the grooves on the surfaces of the teeth are too narrow assessment (CAMBRA) treatment
and deep to clean with a toothbrush. These grooves may decay even if you brush them regularly. protocol guidelines and recom-
Sealants are an excellent preventive measure for children and young adults at risk for this type mendations for children up to
of decay.
age 2; Table 2 lists guidelines and
recommendations for children from
Fig. 4. A parent/caregiver handout: How tooth decay happens. From: Patient information on tooth ages 36. Chlorhexidine rinses, FV,
decay. Available at: http://www.cdafoundation.org/library/docs/jour0303/consensus_forms.pdf. and xylitol-based products may be
( Copyright 2003 by the California Dental Association. Reprinted with permission.) employed to modify the maternal
514 November/December 2010 General Dentistry www.agd.org
Regular dental Family receives Wean off bottle (at least Brush with fluoride toothpaste Only water or
visits for child dental treatment no bottle during sleep) at least twice a day milk in sippy cup
Less or Healthy No soda Chew Drink Less or no candy
no juice snacks xylitol gum tap water or junk food
Check the goals you will focus on between today and your next visit.
On a scale of 110, how confident are you that you can accomplish your goals?
Not likely Definitely
My promise: I agree to the goals checked and understand that staff may ask me how I am doing with my goals.
Important: The last
Date: _______________________ Signed by:______________________________________________ thing that touches your
Review date:__________________ Comments:______________________________ Staff initials:_______ childs teeth before
bedtime is a toothbrush
Review date:__________________ Comments:______________________________ Staff initials:_______ with fluoride toothpaste.
Fig. 5. Self-management goals for parents/caregivers.
transmission of cariogenic bacteria caries risk. Figure 4 presents a form to resistance, schedules follow-up
to infants.16 The risk analysis should that is useful in communicating appointments, and prepares the
allow the caregiver to determine the mechanisms of dental caries parent(s) for the familys specific
any changes that must be made to parents. Their understanding and unique difficulties, which
concerning the childs diet, tooth- of this process is crucial to the inevitably arise when instituting
brushing habits, and fluoride successful implementation of pre- a consistent, lifetime dental care
application. ventive and therapeutic measures.36 program for a child.
Parents should be given addi- A family-centered approach and Following the brief motivational
tional information and anticipatory customized recommendations have interview, the parent/caregiver
guidance on oral health prevention been shown to be more successful is asked to commit to two self-
that is specific to the needs of their in engaging parents to change spe- management goals or recommenda-
child. This information should cific parenting practices than such tions (Fig. 5) and informed that the
include oral hygiene recommenda- generic recommendations such as dentist will discuss these goals at
tions, growth and development brush your teeth twice a day and the childs next appointment.38 The
issues (that is, teething, digit, or dont eat candy.37 form in Figure 6 can be given to
pacifier habits), oral habits, diet and Motivational interviewing (MI) parents as a reminder of their com-
nutrition guidelines, and injury is a counseling technique that mitment to their childs well-being
prevention tips (see Table 3). The relies on two-way communication and can be filed in the childs dental
anticipatory guidance approach is between the clinician and the record, so that the dentist can follow
designed to take advantage of time- patient or parent. MI is meant to up on the familys compliance at
critical opportunities for imple- establish a therapeutic alliance subsequent visits.
menting preventive health practices that is based on rapport and trust.
and thus reduce the childs risk of In this process, the clinician asks Recall visits and periods
preventable oral disease.18 questions to help parents identify Clinicians must consider each childs
During the childs initial visit, problems, listens to their concerns, individual needs to determine the
the dentist must counsel the encourages self-motivational appropriate interval between and
parent(s) to change specific factors statements, prepares them for frequency of oral examinations,
that may be contributing to active change (discussing the hurdles that based on age-specific risk assess-
caries or increasing their childs interfere with action), responds ment and planned treatment. Some
www.agd.org General Dentistry November/December 2010 515
Pediatric Dentistry Caries risk assessment, prevention, and management in pediatric dental care
Parent/caregiver recommendations for control of dental decay and support whenever behavioral
Daily oral hygiene/fluoride toothpaste treatment
changes are required; they should
These procedures reduce the number of bacteria in the mouth and provide a small amount of be questioned about any problems
fluoride to guard against further tooth decay and to repair teeth that display early decay. they might have had following the
Brush childs teeth with a fluoride-containing toothpaste (small smear or pea-sized recommendations. It is essential to
amount on a soft small infant-sized toothbrush) twice daily (gently brushed by parent re-assess the risk status and monitor
or caregiver)
improvement on the previously
Selective daily flossing of teeth with early caries (white spots) set self-management goals. At
Other:____________________________________________________________ every visit, the clinician should
re-evaluate whether it is necessary
Diet
The aim is to reduce the number of between-meal sweet snacks that contain carbohydrates,
to change the recommendations or
especially sugars. Substituting snacks rich in protein, such as cheese, will also help. to continue reinforcing the exist-
OK as is ing prevention protocol. Parents
Limit bottle/nursing (to avoid prolonged contact of milk with teeth) should know that changing dietary
Replace juice or sweet liquids in the bottle with water
and home care practices does not
happen overnight.
Limit snacking (particularly sweets)
Replace high carbohydrate snacks with cheese and protein snacks Summary
Other:____________________________________________________________ General dentists have an important
role in preventing and reducing the
Xylitol (parents/caregivers)
Xylitol is a sweetener that bacteria cannot digest. Using xylitol-containing chewing gum or
severity of ECC in young children.
mints/lozenges is a way for parents/caregivers of children at high risk for caries to reduce the By embracing the concepts of
transfer of decay-causing bacteria to their baby/toddler. This is most effective when used by the dental home and perinatal
the parent/caregiver starting shortly after the child is born. Parents/caregivers with dental and infant oral health, general
decay place their children at high risk for early childhood caries. dentists can implement preventive
Parents/caregivers of children up to the age of 3 who have high bacterial levels should
use xylitol mints/lozenges or xylitol gum two to four times daily.
and treatment protocols in their
practice by using an appropriate,
Antibacterial rinse (parents/caregivers) age-specific caries risk assessment
Parents/caregivers of children at high risk for caries may require antibacterial treatment to instrument to determine the caries
decrease the transmission of cariogenic bacteria and to reduce the infant/childs risk of early risk of their pediatric patients.
childhood caries.
Parents/caregivers of children up to the age of 3 who have high bacterial levels should
rinse with 10 mL of chlorhexidine gluconate 0.12% (by prescription only). Rinse at Acknowledgements
bedtime for one minute once a day for one week. Repeat each month for one week The authors thank Ms. Debra L.
until the infection is controlled. Separate from fluoride use by one hour. Continue for six Tom for her editorial assistance.
months or until bacterial levels remain controlled.
Author information
Practitioner signature: ____________________________________ Date:______________
Dr. Ramos-Gomez is a professor,
Parent/caregiver signature:________________________________ Date:______________ School of Dentistry, University
of California, Los Angeles.
Fig. 6. Parent/caregiver recommendations form. Dr. Crystal is in private practice in
Bound Brook, New Jersey. Dr. Ng
is dentist-in-chief and an assistant
professor, Oral and Developmental
Biology, Harvard School of Dental
infants and toddlers at a high risk for re-evaluation; low-risk children Medicine, Boston, Massachusetts.
for caries should be re-evaluated on should return every 612 months. Dr. Tinanoff is chair, Health
a monthly basis. Most older children After the parents have followed Promotion and Policy, Univer-
at high risk should be seen at three- the recommended protocol for three sity of Maryland in Baltimore.
month intervals for re-evaluation. to six months, they should bring the Dr. Featherstone is a professor and
Children in the moderate risk cat- child back for reassessment. Parents dean, School of Dentistry, Univer-
egory should return every six months need periodic encouragement sity of California, San Francisco.
516 November/December 2010 General Dentistry www.agd.org
References www.aaphd.org/default.asp?page=FirstHealth 27. Featherstone JD. The caries balance: Contribut-
1. Vargas CM, Crall JJ, Schneider DA. Sociodemo- Policy.htm. Accessed July 12, 2010. ing factors and early detection. J Cal Dent Assoc
graphic distribution of pediatric dental caries: 16. Policy on the dental home. Available at: http:// 2003;31(2):129-133.
NHANES III, 1988-1994. J Am Dent Assoc 1988; www.aapd.org/media/Policies_Guidelines/P_ 28. Featherstone JD. The caries balance: The basis
129(9):1229-1238. DentalHome.pdf. Accessed July 12, 2010. for caries management by risk assessment. Oral
2. Poland C 3rd, Hale KJ. Providing oral health to 17. American Academy of Pediatric Dentistry. Policy Health Prev Dent 2004;2 Suppl 1:259-264.
the little ones. J Indiana Dent Assoc 2003;82(4): for early childhood caries (ECC): Classifications, 29. Featherstone JD, Adair SM, Anderson MH,
8-14. consequences and preventive strategies. Pediatr Berkowitz RJ, Bird WF, Crall JJ, Den Besten PK,
3. Health disparities experienced by racial/ethnic Dent 2005-2006;27:31-33. Donly KJ, Glassman P, Milgrom P, Roth JR, Snow
minority populations. MMWR Weekly 2004; 18. American Dental Association. Distribution of R, Stewart RE. Caries management by risk as-
53(33):755. dentists in the United States, by region and sessment: Consensus statement, April 2002. J
4. ADA statement on early childhood caries 2004. state, 2007. Available at: https://www.ada.org/ Calif Dent Assoc 2003;31(3):257-269.
http://www.ada.org/prof/resources/position/ members/ada/prod/survey/07_dod.pdf. Ac- 30. Bijella MF, Bijella VT, Lopes ES, Bastos JR. Com-
caries/. Accessed March 28, 2010. cessed March 30, 2010. parison of dental prophylaxis and toothbrushing
5. The 2006 oral health needs assessment of chil- 19. Keirse M, Plutzer K. Womens attitudes to and prior to topical APF applications. Community
dren. http://www.dentalhealthfoundation.org/ perceptions of oral health and dental care dur- Dent Oral Epidemiol 1985;13(4):208-211.
topics/public/. Accessed April 10, 2007. ing pregnancy. J Perinat Med 2010 38:1,3-8 31. Huebner CE, Riedy CA. Behavioral determinants
6. Macek MD, Wagner ML, Goodman HS, Manz 20. Jiang P, Bargman EP, Garrett NA, DeVries A, of brushing young childrens teeth: Implications
MC, Marrazzo ID. Survey of oral health status of Springman S, Riggs S. A comparison of dental for anticipatory guidance. Pediatr Dent 2010;
Maryland school children, 2000-2001. Pediatr service use among commercially insured 32(1):48-55.
Dent 2004;26(4):329-336. women in Minnesota before, during and after 32. Recommendations for using fluoride to prevent
7. Dye BA, Tan S, Smith V, Lewis BG, Barker LK, pregnancy. J Am Dent Assoc 2008; 139:1173- and control dental caries in the United States.
Thornton-Evans G, et al. Trends in oral health 1180 Centers for Disease Control and Prevention.
status: United States, 19881994 and 1999 21 Thoele MJ, Asche SE, Rindal DB, Fortman KK. MMWR Recomm Rep 2001;50(RR-14):1-42.
2004. Vital Health Stat 11. 2007 Apr;(248): Oral health program preferences among preg- 33. Pang DT, Vann WF Jr. The use of fluoride-con-
1-92. nant women in a managed care organization. J taining toothpastes in young children: The
8. Dye BA, Arevalo O, Vargas CM. Trends in paedi- Public Health Dent 2008;68(3):174-177. scientic evidence for recommending a small
atric dental caries by poverty status in the Unit- 22. Michalowicz BS, DiAngelis AJ, Novak MJ, Bu- quantity. Pediatr Dent 1992;14(6):384-387.
ed States, 19881994 and 19992004. Int J chanan W, Papapanou PN, Mitchell DA, Cur- 34. Amercian Academy of Pediatric Dentistry. AAPD
Paediatr Dent 2010;20:132-143. ran AE, Lupo VR, Ferguson JE, Bofill J, guideline on fluoride therapy, 2009-2010. Avail-
9. Thenisch NL, Bachmann LM, Imfeld T, Leisebach Matseoane S, Deinard AS Jr, Rogers TB. Ex- able from: http://www.aapd.org/media/Policies_
Minder T, Steurer J. Are mutans streptococci de- amining the safety of dental treatment in Guidelines/G_FluorideTherapy.pdf. Last accessed
tected in preschool children a reliable predictive pregnant women. J Am Dent Assoc. 2008 August 10, 2010.
factor for dental caries risk? A systematic re- Jun;139(6):685-95 35. American Dental Association Council on Scien-
view. Caries Res 2006;40(5):366-374. 23. CDA Foundation (2010). Oral health during tific Affairs. Professionally applied topical fluo-
10. Caufield PW, Cutter GR, Dasanayake AP. Initial pregnancy and early childhood: Evidence-based ride. Evidence-based clinical recommendations.
acquisition of mutans streptococci by infants: guidelines for health professionals. Available J Am Dent Assoc 2006;137(8):1151-1159.
Evidence for a discrete window of infectivity. J from: http://www.cdafoundation.org/library/ 36. Featherstone JDB, Domejean-Orliaguet S, Jen-
Dent Res 1993;72(1):37-45. docs/poh_guidelines.pdf. Accessed March 22, son L, Wolff M, Young D. Caries risk assessment
11. Seki M, Yamashita Y, Shibata Y, Torigoe H, Tsu- 2010. in practice for age 6 through adult. J Calif Dent
da H, Maeno M. Effect of mixed mutans strep- 24. Gajendra S, Kumar JV. Oral health and preg- Assoc 2007;35(10):703-712
tococci colonization on caries development. nancy: A review. NY State Dent J 2004;70(1): 37. Weinstein P. Provider versus patient-centered
Oral Microbiol Immunol 2006;21(1):47-52. 40-44. approaches to health promotion with parents of
12. Douglass JM, Li Y, Tinanoff N. Association of mu- 25. Ramos-Gomez FJ. Clinical considerations for an young children: What works/does not work and
tans streptococci between caregivers and their infant oral health care program. Compend Cont why. Pediatr Dent 2006;28(2):172-176.
children. Pediatr Dent 2008;30(5):375-387. Educ Dent 2005;26(5 Suppl 1):17-23. 38. Ramos-Gomez F, Crall J, Slayton R, Featherstone
13. Ramos-Gomez FJ, Bacterial salivary markers 26. American Academy of Pediatric Dentistry. Guide- JD. Caries risk assessment appropriate for the
role in ECC risk assessment in infants. J Dent line on periodicity of examination, preventive age one visit. J Calif Dent Assoc 2007;35(10):
Res Issue 2006;85B:0516. dental services, anticipatory guidance/counsel- 687-702.
14. Nowak AJ. Rationale for the timing of the first ing, and oral treatment for infants, children, and
oral evaluation. Pediatr Dent 1997;19(1):8-11. adolescents. Available at: http://www.aapd.org/ Published with permission by the Academy of
15. American Association of Public Health Dentistry. media/Policies_Guidelines/G_Periodicity.pdf. General Dentistry. Copyright 2010 by the
First oral health assessment policy. 2004. http:// Accessed July 12, 2010. Academy of General Dentistry. All rights reserved.
www.agd.org General Dentistry November/December 2010 517
You might also like
- International Association of Dental Traumatology Guidelines For The Management of Traumatic Dental Injuries: 3. Injuries in The Primary DentitionDocument44 pagesInternational Association of Dental Traumatology Guidelines For The Management of Traumatic Dental Injuries: 3. Injuries in The Primary DentitionaNo ratings yet
- For People With: Ractical Ral Are Developmental DisabilitiesDocument8 pagesFor People With: Ractical Ral Are Developmental DisabilitiesCristian AlberoniNo ratings yet
- Pedo2013 14Document189 pagesPedo2013 14Vladimir Argirovic100% (4)
- Treatment For ChildrenDocument66 pagesTreatment For ChildrenMohsin HabibNo ratings yet
- Tooth DecayDocument17 pagesTooth DecayVictor100% (1)
- Pediatric Dental PatientDocument125 pagesPediatric Dental PatientHebah NawafNo ratings yet
- ABCD PedodontiaDocument120 pagesABCD Pedodontiahridarjunn100% (4)
- Cleft Lip and Palate New ApproachDocument115 pagesCleft Lip and Palate New ApproachsoorajNo ratings yet
- Endomishaps SeminarDocument44 pagesEndomishaps SeminarSuma TettaNo ratings yet
- Nbde01 Examinee GuideDocument36 pagesNbde01 Examinee GuideHKNo ratings yet
- Basic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionFrom EverandBasic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionNo ratings yet
- 4) Epidemiology of Periodontal DiseasesDocument22 pages4) Epidemiology of Periodontal Diseaseswalaa75No ratings yet
- Odontogenic Cysts Summary Chart: Radicular Cyst (Periapical Cyst)Document4 pagesOdontogenic Cysts Summary Chart: Radicular Cyst (Periapical Cyst)ML90No ratings yet
- Endodontic Management of Traumatic InjuriesDocument6 pagesEndodontic Management of Traumatic InjuriesMehwish MunawarNo ratings yet
- Dental Material PDFDocument2 pagesDental Material PDFAbdul Rehman IrfanNo ratings yet
- Dental BiomaterialsDocument491 pagesDental Biomaterialsaris100% (1)
- DAA G1 الجانب الأسنان الأكاديميةDocument253 pagesDAA G1 الجانب الأسنان الأكاديميةnamrata schdevaNo ratings yet
- NSAIDS in Dentistry It's Principles in PracticeDocument6 pagesNSAIDS in Dentistry It's Principles in PracticeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Root CariesDocument17 pagesRoot CariesKhalid Mortaja67% (3)
- Local and Systemic Chemotherapeutic Agents in Periodontics: Part - I Chemical Plaque ControlDocument101 pagesLocal and Systemic Chemotherapeutic Agents in Periodontics: Part - I Chemical Plaque ControlSuresh Bindhumadhav100% (1)
- X-Ray TechniqueDocument48 pagesX-Ray Techniquesohaksa bashaNo ratings yet
- TMJ PDFDocument3 pagesTMJ PDFParneetNo ratings yet
- Oxford Assess and Progress Clinical DentistryDocument361 pagesOxford Assess and Progress Clinical Dentistrysmustafa.officeNo ratings yet
- CHAPTER 13. Interdisciplinary ConsiderationsDocument13 pagesCHAPTER 13. Interdisciplinary ConsiderationsAlina AnechiteiNo ratings yet
- Pedo MCQs QuestionsDocument17 pagesPedo MCQs QuestionsYazan Emad Salem90% (30)
- Microsurgery in EndodonticsFrom EverandMicrosurgery in EndodonticsSyngcuk KimNo ratings yet
- Oral Biologic Defenses in Tooth Demineralization and RemineralizationDocument14 pagesOral Biologic Defenses in Tooth Demineralization and RemineralizationWilson Fransiskus Chia GirsangNo ratings yet
- Bone Loss PatternsDocument36 pagesBone Loss PatternsMavis100% (1)
- NEET MDS Mock TestDocument158 pagesNEET MDS Mock TestAysha NazrinNo ratings yet
- Diet and Dental CariesDocument105 pagesDiet and Dental Cariesdentistpro.org100% (1)
- Advanced Microbial Diagnostic Techniques in PeriodonticsDocument38 pagesAdvanced Microbial Diagnostic Techniques in PeriodonticsPiyusha SharmaNo ratings yet
- Acute Periodontal LesionsDocument30 pagesAcute Periodontal LesionsJorge CabreraNo ratings yet
- Teeth Eruption WordDocument24 pagesTeeth Eruption WordAhmed hegazyNo ratings yet
- Section 1 Introduction: Evolution of Caries Treatment Approaches and Comorbidity With Systemic Health ProblemsDocument10 pagesSection 1 Introduction: Evolution of Caries Treatment Approaches and Comorbidity With Systemic Health ProblemsAnggita Dwi PutriNo ratings yet
- Caries Activity TestDocument19 pagesCaries Activity TestArizona GreyNo ratings yet
- Caries Activity TestDocument19 pagesCaries Activity TestArizona GreyNo ratings yet
- Perio Case History 2Document86 pagesPerio Case History 2Moola Bharath Reddy100% (1)
- Epidemiologi Dental CariesDocument21 pagesEpidemiologi Dental CariesSampahAjaNo ratings yet
- 03 MFDS Regulations & Syllabus 2011Document15 pages03 MFDS Regulations & Syllabus 2011FarahMohammed1No ratings yet
- Dentine HypersensitivityDocument32 pagesDentine Hypersensitivityitdoc100% (1)
- International Caries Detection and Assessment System (ICDAS) PDFDocument4 pagesInternational Caries Detection and Assessment System (ICDAS) PDFKelvin Jaya AlamNo ratings yet
- Department of Pedodontics: Submitted By: Shayoni Sen Bds Ivth YearDocument29 pagesDepartment of Pedodontics: Submitted By: Shayoni Sen Bds Ivth YearFarzana ShereenNo ratings yet
- FlipchartDocument14 pagesFlipchartapi-508053077No ratings yet
- 1st Course Introductory Course in Paediatric Dentistry&Childhood StagesDocument29 pages1st Course Introductory Course in Paediatric Dentistry&Childhood StagesChristosSougkakisNo ratings yet
- Effect of Tongue Brushing On Oral Malodor in AdolescentsDocument5 pagesEffect of Tongue Brushing On Oral Malodor in AdolescentsMarian Si Teofana HasnaNo ratings yet
- Maintenance of Space by Innovative Three-DimensionDocument4 pagesMaintenance of Space by Innovative Three-DimensionhenariaNo ratings yet
- Molar Incisor Hypomineralization Supplementary, Restorative, Orthodontic, and Esthetic Long-Term Treatment 2019Document6 pagesMolar Incisor Hypomineralization Supplementary, Restorative, Orthodontic, and Esthetic Long-Term Treatment 2019player osamaNo ratings yet
- Gingival Diseases - Their Aetiology, Prevention and Treatment PDFDocument246 pagesGingival Diseases - Their Aetiology, Prevention and Treatment PDFnaresh sharma0% (1)
- Dental Plaque: By:-Raina J. P. Khanam Post Graduate 2 Year Dept. of Periodontics and ImplantologyDocument69 pagesDental Plaque: By:-Raina J. P. Khanam Post Graduate 2 Year Dept. of Periodontics and ImplantologyAtul KoundelNo ratings yet
- Dental HygieneDocument3 pagesDental Hygieneapi-507354264No ratings yet
- Geriatric Oral HealthDocument12 pagesGeriatric Oral HealthCeza CezaaNo ratings yet
- Introduction To DentistryDocument30 pagesIntroduction To DentistryĐỗ Thành KhangNo ratings yet
- Evidence Based DentistryDocument5 pagesEvidence Based DentistrySaumyaGc_singhNo ratings yet
- Dentin Hypersensitivity2 PDFDocument5 pagesDentin Hypersensitivity2 PDFIvan TerresNo ratings yet
- Data Sufficiency Part - 2Document29 pagesData Sufficiency Part - 2dharmsmart19No ratings yet
- Curretage Laser Vs ConventionalDocument5 pagesCurretage Laser Vs ConventionalVembri IrawatiNo ratings yet
- Recent Advancements in Restorative Dentistry: An OverviewDocument9 pagesRecent Advancements in Restorative Dentistry: An Overviewadnan ghNo ratings yet
- Silver Diamine Fluoride - A Futuristic Remedy For Caries TerminationDocument5 pagesSilver Diamine Fluoride - A Futuristic Remedy For Caries TerminationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- OMD411T - Oral Medicine 1Document117 pagesOMD411T - Oral Medicine 1Noura Rihan100% (1)
- Pediatric DentistryDocument15 pagesPediatric Dentistrymirfanulhaq100% (2)
- Space Maintenance: Emma Laing, Paul Ashley, Farhad B. Naini & Daljit S. GillDocument8 pagesSpace Maintenance: Emma Laing, Paul Ashley, Farhad B. Naini & Daljit S. GillAnonymous JR1VNCNo ratings yet
- Success& Failures in EndoDocument32 pagesSuccess& Failures in Endorasagna reddyNo ratings yet
- Part1bco Mmmntent1Document4 pagesPart1bco Mmmntent1Zain KolachiNo ratings yet
- L4 Kranthi PPT Icdas IIDocument59 pagesL4 Kranthi PPT Icdas IIsheryl teoNo ratings yet
- Pangan, Maria Elaine S. Inlay Onlay GoldDocument6 pagesPangan, Maria Elaine S. Inlay Onlay GoldErika PanganNo ratings yet
- ADEA Dental School Admission Timelines Costs and TipsDocument8 pagesADEA Dental School Admission Timelines Costs and Tipsejl09No ratings yet
- My Dentist and the Tooth Fairy: Activity and Coloring BookFrom EverandMy Dentist and the Tooth Fairy: Activity and Coloring BookNo ratings yet
- Topical Drugs in DentistryDocument6 pagesTopical Drugs in DentistryIyad Abou-RabiiNo ratings yet
- Oral Health Care in ChildrenDocument2 pagesOral Health Care in ChildrenRaul GhiurcaNo ratings yet
- DMG Catalog DentalDocument64 pagesDMG Catalog DentalErdeli StefaniaNo ratings yet
- Effect of 5% Fluoride Varnish Application On Caries Among School Children in Rural BrazilDocument11 pagesEffect of 5% Fluoride Varnish Application On Caries Among School Children in Rural BrazilAhmad Ulil AlbabNo ratings yet
- 04-14-08 Application of F and CaPDocument8 pages04-14-08 Application of F and CaPvelangniNo ratings yet
- Guideline On Dental Management of Pediatric Patients Receiving Chemotherapy, Hematopoietic Cell Transplantation, And:Or Radiation TherapyDocument9 pagesGuideline On Dental Management of Pediatric Patients Receiving Chemotherapy, Hematopoietic Cell Transplantation, And:Or Radiation TherapyasdatNo ratings yet
- The Huddle 5-18-15 EDITDocument4 pagesThe Huddle 5-18-15 EDITSarah DoyleNo ratings yet
- Dental Provider's Oncology Pocket Guide: Special Care For ChildrenDocument10 pagesDental Provider's Oncology Pocket Guide: Special Care For Childrenمحمد عبدالهادي إسماعيلNo ratings yet
- Changing Concepts in Cariology - Forty Years OnDocument7 pagesChanging Concepts in Cariology - Forty Years OnDavid CaminoNo ratings yet
- Hele Grade4Document56 pagesHele Grade4Chard Gonzales100% (3)
- (Đề thi có 05 trang) : Thời gian làm bài: 60 phút; không kể thời gian phát đềDocument5 pages(Đề thi có 05 trang) : Thời gian làm bài: 60 phút; không kể thời gian phát đềTrịnh YếnNo ratings yet
- KDJVol35No4 KeralaDentalJournalDocument75 pagesKDJVol35No4 KeralaDentalJournalIndrani Das50% (2)
- Simultaneous Removal of Hardness and Fluoride by Electrocoagulation and Chemical CoagulationDocument50 pagesSimultaneous Removal of Hardness and Fluoride by Electrocoagulation and Chemical CoagulationMahammed PalagiriNo ratings yet
- Short GuidelinesDocument52 pagesShort GuidelinesMohamed FaizalNo ratings yet
- Test 6Document6 pagesTest 6Minhh Huyenn VuNo ratings yet
- 01Document142 pages01Praveena SailenthranNo ratings yet
- Tooth Decay Easy Read GuideDocument29 pagesTooth Decay Easy Read GuideSTEM JordanNo ratings yet
- Guideline On Behavior Guidance For The Pediatric Dental PatientDocument13 pagesGuideline On Behavior Guidance For The Pediatric Dental PatientPriscila Belén Chuhuaicura SotoNo ratings yet
- Effective Interventions To Prevent Dental Caries in Preschool ChildrenDocument56 pagesEffective Interventions To Prevent Dental Caries in Preschool ChildrenDiego AzaedoNo ratings yet
- When To Intervene in The Caries Process? An Expert Delphi Consensus StatementDocument13 pagesWhen To Intervene in The Caries Process? An Expert Delphi Consensus StatementPablo BenitezNo ratings yet
- Fluoride TherapyDocument4 pagesFluoride TherapyمعتزباللهNo ratings yet