You might also like
- Corporate Compliance Programs Plans-2Document7 pagesCorporate Compliance Programs Plans-2WilliamArugaNo ratings yet
- Hospital ComplianceDocument15 pagesHospital ComplianceStella HerliantineNo ratings yet
- Manpower Planning & Resourcing Mu001 B0816Document11 pagesManpower Planning & Resourcing Mu001 B0816anithanhNo ratings yet
- Accounts Payable Job ProfileDocument2 pagesAccounts Payable Job ProfileChester LowbyteNo ratings yet
- Employee Turnover ProceduresDocument9 pagesEmployee Turnover ProceduresDuaa KhanNo ratings yet
- Competency Framework - ManufactureDocument7 pagesCompetency Framework - ManufactureTai BausekaliNo ratings yet
- Competency MappingDocument45 pagesCompetency MappingnamrataNo ratings yet
- Continuous Quality Improvement Techniques: Introduction ToDocument47 pagesContinuous Quality Improvement Techniques: Introduction ToParameswara Rao KoutarapuNo ratings yet
- Job Evaluation Point MethodDocument10 pagesJob Evaluation Point MethodchaselionNo ratings yet
- Hay JE Overview-General DistributionDocument18 pagesHay JE Overview-General DistributionmmfaruqNo ratings yet
- Kano Model - Term PaperDocument13 pagesKano Model - Term PaperCatherine WekesaNo ratings yet
- Organizational StructureDocument26 pagesOrganizational StructureSahanaa AJNo ratings yet
- Compensation ManagementDocument45 pagesCompensation ManagementAjjarapu JaikaliprasadNo ratings yet
- Report On CompensationDocument40 pagesReport On CompensationtomalNo ratings yet
- Strong Governance PracticesDocument26 pagesStrong Governance PracticesPrasad GantiNo ratings yet
- Quality Control (QC) Matrix Skill Certificate: (Name) (ID)Document1 pageQuality Control (QC) Matrix Skill Certificate: (Name) (ID)Linda Setya WatiNo ratings yet
- Contents of Synopsis: A Study On Job Roles at "Infiniti Building Solutions Private Limited"Document7 pagesContents of Synopsis: A Study On Job Roles at "Infiniti Building Solutions Private Limited"Gyaneshwar CHNo ratings yet
- Job Evaluation: Ranking Method RankDocument4 pagesJob Evaluation: Ranking Method RankJariNo ratings yet
- Occupational Hygiene Procedure - Sew19Document19 pagesOccupational Hygiene Procedure - Sew19abdulla kasimNo ratings yet
- A Study On Recuritment at Axiom TechnologiesDocument7 pagesA Study On Recuritment at Axiom TechnologiessrikanthNo ratings yet
- To Run in Slide Show ModeDocument29 pagesTo Run in Slide Show Modeaayush007No ratings yet
- 3.job EvaluationDocument12 pages3.job EvaluationEllen NegrilloNo ratings yet
- JVH PHANI Performance Review System Mba HR ProjecDocument49 pagesJVH PHANI Performance Review System Mba HR ProjecKRISHNA SASTRYNo ratings yet
- Job Analysis ConsultancyDocument2 pagesJob Analysis Consultancypeter mulilaNo ratings yet
- Delegation of Authority: Duluxgroup LimitedDocument7 pagesDelegation of Authority: Duluxgroup LimitedGaurav WadhwaNo ratings yet
- Job EvaluationDocument15 pagesJob EvaluationAnkur DubeyNo ratings yet
- Operations Risk Paper - Dec 2011Document24 pagesOperations Risk Paper - Dec 2011Lis SuryaniNo ratings yet
- JD Logistics ManagerDocument3 pagesJD Logistics ManagerRubayetNo ratings yet
- Bench SawDocument4 pagesBench SawimranNo ratings yet
- Module 1Document17 pagesModule 1buviaroNo ratings yet
- Compensation: Third Canadian Edition Milkovich, Newman, ColeDocument28 pagesCompensation: Third Canadian Edition Milkovich, Newman, ColeNeha AgarwalNo ratings yet
- Failure Mode and Effect Analysis - FMEADocument64 pagesFailure Mode and Effect Analysis - FMEAtanto_deep_15No ratings yet
- Building Emergency Action Plan (BEAP)Document5 pagesBuilding Emergency Action Plan (BEAP)nyan linNo ratings yet
- Skills-Audit-Document - Docx1Document14 pagesSkills-Audit-Document - Docx1api-318111074No ratings yet
- JOB Defined JOB Description JOB Analysis JOB Specification JOB EvaluationDocument99 pagesJOB Defined JOB Description JOB Analysis JOB Specification JOB EvaluationAshish GuptaNo ratings yet
- Apics-Pdm Using PdcaDocument50 pagesApics-Pdm Using Pdcaernesto_jerez_1No ratings yet
- Assignment - 4Document23 pagesAssignment - 4lekha magantiNo ratings yet
- Business Process ModellingDocument3 pagesBusiness Process ModellingAbhimanyu ChoudharyNo ratings yet
- Akshay Offer LetterDocument4 pagesAkshay Offer LetterAkshay SinghNo ratings yet
- CS3 App Dev CompetencyDocument10 pagesCS3 App Dev CompetencyPKNo ratings yet
- Competency ManagersDocument25 pagesCompetency ManagersSalatino RenataNo ratings yet
- Employee GrievancesDocument37 pagesEmployee Grievancesravikiran1231No ratings yet
- How To Design An Organization StructureDocument3 pagesHow To Design An Organization StructureShereen HossamNo ratings yet
- Skill Audit ProcessDocument2 pagesSkill Audit ProcessthrinadNo ratings yet
- Performance AppraisalDocument81 pagesPerformance AppraisalIkhlaasKaushalNo ratings yet
- Job Evaluation ManualDocument12 pagesJob Evaluation Manualrendra_permana4585No ratings yet
- Presentation On Internal AlignmentDocument24 pagesPresentation On Internal AlignmentAman KaurNo ratings yet
- Best Practice SOX ComplinceDocument8 pagesBest Practice SOX ComplinceSundar KumarNo ratings yet
- Employee Performance Appraisal SampleDocument6 pagesEmployee Performance Appraisal SampleLydia ThompsonNo ratings yet
- Allocating T & D ResourcesDocument23 pagesAllocating T & D ResourcesEkta Sandeep SharmaNo ratings yet
- Work Study (Case Study) PresentationDocument36 pagesWork Study (Case Study) PresentationMeet JaiswalNo ratings yet
- Evaluating Employee PerformanceDocument12 pagesEvaluating Employee PerformancenurfitriaNo ratings yet
- Atex DirectiveDocument4 pagesAtex DirectiveMichaelNo ratings yet
- SCRIPT Competency Framework Dictionary-EnglishDocument9 pagesSCRIPT Competency Framework Dictionary-EnglishfasihNo ratings yet
- Sample Report of KYKO Personality Profile For Competency ManagementDocument23 pagesSample Report of KYKO Personality Profile For Competency ManagementBernard Ah Thau TanNo ratings yet
- Textbook of Urgent Care Management: Chapter 21, Employment Contracts and CompensationFrom EverandTextbook of Urgent Care Management: Chapter 21, Employment Contracts and CompensationNo ratings yet
- Textbook of Urgent Care Management: Chapter 37, Setting Up a Health-Care Compliance ProgamFrom EverandTextbook of Urgent Care Management: Chapter 37, Setting Up a Health-Care Compliance ProgamNo ratings yet
- ComforceHealth ComplianceDocument14 pagesComforceHealth ComplianceVintiNo ratings yet
- Compliance Work PlanDocument4 pagesCompliance Work PlanayaNo ratings yet
- DGP00673AAA Issue 1-04 GSS4100 User ManualDocument149 pagesDGP00673AAA Issue 1-04 GSS4100 User ManualrmNo ratings yet
- Contractor Quality Control Plan Free Word Template DownloadDocument30 pagesContractor Quality Control Plan Free Word Template DownloadrmNo ratings yet
- Azure Sphere Bootcamp Overview With AgendaDocument1 pageAzure Sphere Bootcamp Overview With AgendarmNo ratings yet
- Pmp20122 Rev B Bill of Materials: Designator Quantity Value Partnumber Manufacturer Description PackagereferenceDocument2 pagesPmp20122 Rev B Bill of Materials: Designator Quantity Value Partnumber Manufacturer Description PackagereferencermNo ratings yet
- LoRa Start 20181113 - NDDocument4 pagesLoRa Start 20181113 - NDrmNo ratings yet
- TAJ Series: Standard TantalumDocument7 pagesTAJ Series: Standard TantalumrmNo ratings yet
- U.S. EPA Templates For Creating A National GHG Inventory System ManualDocument26 pagesU.S. EPA Templates For Creating A National GHG Inventory System ManualrmNo ratings yet
- RST User: Lora Node 151 Pinout DiagramDocument1 pageRST User: Lora Node 151 Pinout DiagramrmNo ratings yet
- Qa-Checklist Final 2005 0Document10 pagesQa-Checklist Final 2005 0rmNo ratings yet
- D&D Essentials Kit Scribd 2Document6 pagesD&D Essentials Kit Scribd 2rm50% (2)
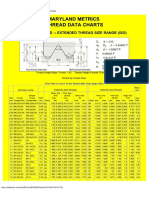
- Metric Thread PG 1Document1 pageMetric Thread PG 1rmNo ratings yet
- Designing Ultrafast Loop Response With Type-III Compensation For Current Mode Step-Down ConvertersDocument9 pagesDesigning Ultrafast Loop Response With Type-III Compensation For Current Mode Step-Down ConvertersrmNo ratings yet
- D&D Essentials Kit Scribd 1Document5 pagesD&D Essentials Kit Scribd 1rm25% (8)
- WE CBT Webinar Plugging ENDocument15 pagesWE CBT Webinar Plugging ENrmNo ratings yet
- Product Development Processes: Prof. Olivier de WeckDocument27 pagesProduct Development Processes: Prof. Olivier de WeckrmNo ratings yet
- Esp32 Azure Iot Kit Hardware Design GuideDocument11 pagesEsp32 Azure Iot Kit Hardware Design GuidermNo ratings yet
- DETC2011-48125 DETC2011-4: An Ontology of Classification Criteria For Functional TaxonomiesDocument10 pagesDETC2011-48125 DETC2011-4: An Ontology of Classification Criteria For Functional TaxonomiesrmNo ratings yet
- FPR de Weck Jul 1 2012Document59 pagesFPR de Weck Jul 1 2012rmNo ratings yet
- People v. CerdonDocument3 pagesPeople v. CerdonChimney sweepNo ratings yet
- Sourav Panda e Commerce PresenationDocument10 pagesSourav Panda e Commerce Presenationsourav pandaNo ratings yet
- Searle Institution Seminario 2006 04dDocument22 pagesSearle Institution Seminario 2006 04dchepiruloNo ratings yet
- Mou Work ImmersionDocument6 pagesMou Work ImmersionMarlou GayaneloNo ratings yet
- Ok Business Law & Ethics-1Document2 pagesOk Business Law & Ethics-1Tanish ReddyNo ratings yet
- E-Goverment Opportunities and ChallengesDocument24 pagesE-Goverment Opportunities and ChallengesMikaye WrightNo ratings yet
- Amigo Manufacturing Inc., V. Cluett Peabody G.R. No. 139300 March 14, 2001Document2 pagesAmigo Manufacturing Inc., V. Cluett Peabody G.R. No. 139300 March 14, 2001Konrad IbabaoNo ratings yet
- Mathematics of LotteriesDocument339 pagesMathematics of LotteriesJose Estrada100% (3)
- Energy Management Solutions - CatalogueDocument56 pagesEnergy Management Solutions - CatalogueShilpa GharatNo ratings yet
- SSM English CatalogueDocument196 pagesSSM English CatalogueSELCUK ONUKNo ratings yet
- Dobrolyubov On EducationDocument19 pagesDobrolyubov On EducationVladi IlichNo ratings yet
- HR Audit ChecklistDocument4 pagesHR Audit Checklistpielzapa50% (2)
- Sample of Consignment Format PDFDocument1 pageSample of Consignment Format PDFBeatrice JayNo ratings yet
- NSCP 2015Document1,032 pagesNSCP 2015Rouzurin Ross100% (1)
- Example Network DesignDocument41 pagesExample Network DesignmichaelnancarrowNo ratings yet
- Life Cycle Assessment of Electricity Generation in Mauritius - SIMAPRO PDFDocument11 pagesLife Cycle Assessment of Electricity Generation in Mauritius - SIMAPRO PDFLeonardo Caldas100% (1)
- Viral Vankadiya Assignment 2Document2 pagesViral Vankadiya Assignment 2Viral PatelNo ratings yet
- Basic AccountsDocument51 pagesBasic AccountsNilesh Indikar100% (1)
- Menu Standart Altas CateringDocument13 pagesMenu Standart Altas CateringAlam almadaniNo ratings yet
- Na Mono Lage Na - Na Jiya Lage Na - Text - LyricsDocument4 pagesNa Mono Lage Na - Na Jiya Lage Na - Text - Lyricsapi-372531067% (3)
- Cost of Doing BusinessDocument5 pagesCost of Doing BusinessmysubicbayNo ratings yet
- PEP Web - Ernst Simmel and Freudian PhilosophyDocument3 pagesPEP Web - Ernst Simmel and Freudian Philosophyrogne100% (1)
- Ib History HL Revision Work BookDocument69 pagesIb History HL Revision Work Bookapi-239922881No ratings yet
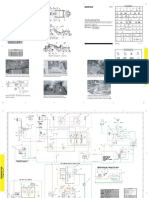
- Esquema Hidráulico Trailla 631GDocument2 pagesEsquema Hidráulico Trailla 631GJose Carlos Annicchiarico BritoNo ratings yet
- Cave of Iapodes-An Early Slavic Shrine of Perun-KresnikDocument16 pagesCave of Iapodes-An Early Slavic Shrine of Perun-KresnikprevisetraziteNo ratings yet
- Seattle Parents File Wrongful Death Lawsuit Against Greyhound in The Death of Their Son - PLFS' Orig Pet (File-Marked 12-05-17)Document13 pagesSeattle Parents File Wrongful Death Lawsuit Against Greyhound in The Death of Their Son - PLFS' Orig Pet (File-Marked 12-05-17)Androvett Legal MediaNo ratings yet
- Power Plant Engineering - The NewDocument9 pagesPower Plant Engineering - The NewSafaa Hameed Al NaseryNo ratings yet
- Iau Interview Call Letter BangaloreDocument2 pagesIau Interview Call Letter BangaloreAyaan HashimNo ratings yet
- News WritingDocument41 pagesNews WritingNovelyn Ramos TunogNo ratings yet
- The Mayor of Casterbridge: What's InsideDocument35 pagesThe Mayor of Casterbridge: What's Insidemdms100% (1)