You might also like
- A Fascia and The Fascial SystemDocument2 pagesA Fascia and The Fascial SystemGriNo ratings yet
- Interfascial Plane Blocks BasicsDocument6 pagesInterfascial Plane Blocks BasicskritziaNo ratings yet
- Plasticity FascialDocument13 pagesPlasticity FascialMichael DuranNo ratings yet
- Elsa Lindenberg and ReichDocument22 pagesElsa Lindenberg and ReichRoberto RosaNo ratings yet
- Critically Evaluate The Development of Irish Law On The Duty of Decision-Makers To Give Reasons For Their Decisions.Document11 pagesCritically Evaluate The Development of Irish Law On The Duty of Decision-Makers To Give Reasons For Their Decisions.Philip Reynor Jr.No ratings yet
- Bio Dynamics The Fascia of The Pelvic Floor Model of TensegrityDocument8 pagesBio Dynamics The Fascia of The Pelvic Floor Model of TensegritygabrielsantosmsNo ratings yet
- Paxton Contact ImprovisationDocument4 pagesPaxton Contact ImprovisationRAFAEL VICENT ARNAL RODRIGONo ratings yet
- The Fascia As Organ of Innerness 2015 EN ChapterDocument16 pagesThe Fascia As Organ of Innerness 2015 EN ChapterJorge Flores TorresNo ratings yet
- Lecture Notes On Psoas & Adductors: Psoas As A Medial RotatorDocument12 pagesLecture Notes On Psoas & Adductors: Psoas As A Medial RotatorAlisaClark100% (1)
- 0418MC 04.17.19 Form 25 CPM Flagging Checklist 28th STDocument3 pages0418MC 04.17.19 Form 25 CPM Flagging Checklist 28th STMohammed Jahanzeb ChoudaryNo ratings yet
- TikTok - Make Your Day 8-8 3Document49 pagesTikTok - Make Your Day 8-8 3Lakotre 129No ratings yet
- Brain Sciences: Biological, Psychological, and Social Determinants of Depression: A Review of Recent LiteratureDocument33 pagesBrain Sciences: Biological, Psychological, and Social Determinants of Depression: A Review of Recent LiteratureGulliver EsoyNo ratings yet
- Research About Lemon GrassDocument19 pagesResearch About Lemon GrassMary Jane Olpindo0% (1)
- Body Schema Building During Childhood and AdolescenceDocument10 pagesBody Schema Building During Childhood and AdolescenceAída MoraNo ratings yet
- Diri Journal March 2022 Interactive 2Document91 pagesDiri Journal March 2022 Interactive 2bfbernardesNo ratings yet
- Cranial Rhythmic Impulse Related To The Traube-Hering-Mayer OscillationDocument11 pagesCranial Rhythmic Impulse Related To The Traube-Hering-Mayer Oscillationthe_walnutNo ratings yet
- A Model of Human Postural Control Inspired by Separated Human Sensory SystemsDocument10 pagesA Model of Human Postural Control Inspired by Separated Human Sensory SystemspamelaNo ratings yet
- Land Law Problem QuestionDocument9 pagesLand Law Problem QuestionPhilip Reynor Jr.No ratings yet
- Husserl - Kant and The Idea of Transcendental PhilosophyDocument26 pagesHusserl - Kant and The Idea of Transcendental PhilosophyPhilip Reynor Jr.No ratings yet
- Single Phase Induction MotorsDocument11 pagesSingle Phase Induction MotorsSafnas KariapperNo ratings yet
- 1.temporal Bone & Skull Base Anatomy Seminar 1Document67 pages1.temporal Bone & Skull Base Anatomy Seminar 1fitsumalemayehudNo ratings yet
- John Rolland - Inside MotionDocument154 pagesJohn Rolland - Inside MotionAnisoara Cismasu100% (3)
- The Body's Insistence On Meaning: Metaphor As Presentation and Representation in Illness ExperienceDocument25 pagesThe Body's Insistence On Meaning: Metaphor As Presentation and Representation in Illness ExperienceNaphtali Gaither100% (1)
- Making Sense of ProprioceptionDocument10 pagesMaking Sense of Proprioceptionjuanito1979No ratings yet
- FasciaDocument12 pagesFasciaRodolfo CiqueleiroNo ratings yet
- Conscious Mind Conscious BodyDocument26 pagesConscious Mind Conscious Bodynikos kasiktsisNo ratings yet
- Sass - Heidegger Schizophrenia and The Ontological DifferenceDocument25 pagesSass - Heidegger Schizophrenia and The Ontological DifferencePhilip Reynor Jr.No ratings yet
- Pain and NeuromatrixDocument5 pagesPain and NeuromatrixBharathGopinathNo ratings yet
- 24 - Proprioception and Neuromuscular ControlDocument24 pages24 - Proprioception and Neuromuscular ControlCarlos Garcia100% (2)
- Bones & Joints of Head & NeckDocument91 pagesBones & Joints of Head & NeckSalman KhanNo ratings yet
- Revealing The Hidden: The Epiphanic Dimension of Games and SportDocument31 pagesRevealing The Hidden: The Epiphanic Dimension of Games and SportXimena BantarNo ratings yet
- The Kinesthetic SystemDocument8 pagesThe Kinesthetic SystemCANDELA SALGADO IVANICHNo ratings yet
- Student Guidance.Document78 pagesStudent Guidance.Meghan TaylorNo ratings yet
- Cranial NervesDocument16 pagesCranial Nervesapi-302547403100% (1)
- The Signficance of RespirationDocument12 pagesThe Signficance of RespirationApril Dawn100% (1)
- The M. Steiner Collection of Stringed InstrumentsDocument178 pagesThe M. Steiner Collection of Stringed InstrumentskoutetsuNo ratings yet
- Zahavi 1998 - The Fracture in Self AwarenessDocument15 pagesZahavi 1998 - The Fracture in Self AwarenessPhilip Reynor Jr.100% (1)
- Differences, Vol 6, No 2-3 (2011) - The Sense of SoundDocument329 pagesDifferences, Vol 6, No 2-3 (2011) - The Sense of SoundvictorNo ratings yet
- Zahavi Dan Husserl S Phenomenology PDFDocument188 pagesZahavi Dan Husserl S Phenomenology PDFManuel Pepo Salfate50% (2)
- ButohDocument10 pagesButohShilpa AlaghNo ratings yet
- Sass & Parnas - Schizophrenia, Consciousness, and The SelfDocument18 pagesSass & Parnas - Schizophrenia, Consciousness, and The SelfPhilip Reynor Jr.No ratings yet
- Alweiss - The World UnclaimedDocument266 pagesAlweiss - The World UnclaimedPhilip Reynor Jr.No ratings yet
- MindOutsideBrain HeylighenandBeigi1Document24 pagesMindOutsideBrain HeylighenandBeigi1Taziita LOreleyNo ratings yet
- Husserl - Vienna LectureDocument27 pagesHusserl - Vienna LecturePhilip Reynor Jr.No ratings yet
- The Occipital BoneDocument5 pagesThe Occipital Boneinna3003No ratings yet
- Bobath For Musculoskeletal Problem Palembang Online 2020Document128 pagesBobath For Musculoskeletal Problem Palembang Online 2020fisioterapi rsph100% (1)
- Husserl - Encyclopedia Britannica ArticleDocument14 pagesHusserl - Encyclopedia Britannica ArticlePhilip Reynor Jr.100% (1)
- Husserl - Phenomenology and Anthropology (1931)Document21 pagesHusserl - Phenomenology and Anthropology (1931)Philip Reynor Jr.100% (2)
- Nigeria Rice Value ChainDocument57 pagesNigeria Rice Value ChainAndres Felipe Garcia71% (7)
- The Cranial Bowl in The New Millennium and Sutherland's Legacy For Osteopathic Medicine: Part 1Document9 pagesThe Cranial Bowl in The New Millennium and Sutherland's Legacy For Osteopathic Medicine: Part 1Juanillo CraneosacralNo ratings yet
- Kevin Frank - Body - As - A - Movement - SystemDocument10 pagesKevin Frank - Body - As - A - Movement - Systemleo100% (1)
- Embodied Enactive DMT - Por Sabien C. Koch y Diana FischmanDocument16 pagesEmbodied Enactive DMT - Por Sabien C. Koch y Diana Fischmanroselita321No ratings yet
- Bige 2017 Tonic Space PDFDocument5 pagesBige 2017 Tonic Space PDFRomain BigéNo ratings yet
- Carman - The Body in Husserl and Merleau-PontyDocument22 pagesCarman - The Body in Husserl and Merleau-PontyRené AramayoNo ratings yet
- Bigé&godard 2019 Moving Moved PDFDocument20 pagesBigé&godard 2019 Moving Moved PDFRomain Bigé100% (1)
- The Organ of Form: Towards A Theory of Biological ShapeDocument11 pagesThe Organ of Form: Towards A Theory of Biological Shapesusanne voraNo ratings yet
- Intentionality and The Phenomenology of ActionDocument15 pagesIntentionality and The Phenomenology of Actionherac12100% (1)
- Husserl - Amsterdam LecturesDocument13 pagesHusserl - Amsterdam LecturesPhilip Reynor Jr.No ratings yet
- Lauer 1979 Book The Triumph of SubjectivityDocument192 pagesLauer 1979 Book The Triumph of Subjectivityhassan_hamoNo ratings yet
- Husserl - Philosophy As A Rigorous Science (New Translation)Document47 pagesHusserl - Philosophy As A Rigorous Science (New Translation)Philip Reynor Jr.84% (19)
- SomaticsDocument15 pagesSomaticsAicha Ruxandra100% (1)
- Artigo - Art and BrainDocument20 pagesArtigo - Art and BrainJosé Augusto Rento CardosoNo ratings yet
- Neurostructural Integration Technique: A Better Way To Good Health! Michael J. Nixon-LivyDocument66 pagesNeurostructural Integration Technique: A Better Way To Good Health! Michael J. Nixon-Livytheodora_bobes100% (1)
- EU Law Problem Question - Direct Effect, Indirect Effect and Incidental Horizontal EffectDocument13 pagesEU Law Problem Question - Direct Effect, Indirect Effect and Incidental Horizontal EffectPhilip Reynor Jr.60% (5)
- Design of Lining of Tunnels Excavated in Soil and Soft Rock PDFDocument15 pagesDesign of Lining of Tunnels Excavated in Soil and Soft Rock PDFtradichon23No ratings yet
- Steve Paxton TranscriptDocument24 pagesSteve Paxton Transcriptapi-469504237No ratings yet
- The Brain's Sense of Movement - Alan BerthozDocument352 pagesThe Brain's Sense of Movement - Alan BerthozKaroline MarxNo ratings yet
- Well Kill MethodsDocument3 pagesWell Kill MethodsCARLOSELSOARESNo ratings yet
- ProprioceptionDocument142 pagesProprioceptionssanagavNo ratings yet
- A Neuropsychoanalytic Viewpoint: Commentary On Paper by Steven H. KnoblauchDocument26 pagesA Neuropsychoanalytic Viewpoint: Commentary On Paper by Steven H. KnoblauchPaul ScallanNo ratings yet
- Jeremy Bentham, Legal Positivism, Utilitariamism and The PanopticonDocument10 pagesJeremy Bentham, Legal Positivism, Utilitariamism and The PanopticonPhilip Reynor Jr.100% (1)
- Clark - Embodiment and The Philosophy of MindDocument29 pagesClark - Embodiment and The Philosophy of MindPhilip Reynor Jr.No ratings yet
- Onur Karamercan, Merleau-Ponty, PerceptionDocument12 pagesOnur Karamercan, Merleau-Ponty, Perceptionmentologist100% (1)
- When Body Image Takes Over The Body Schema The CaseDocument13 pagesWhen Body Image Takes Over The Body Schema The CaseMauro Torres100% (1)
- Postdramatic Theatre (Review) - Jeanne WillcoxonDocument3 pagesPostdramatic Theatre (Review) - Jeanne WillcoxonBülent GültekinNo ratings yet
- ReeducationSensorimotor PrinciplesandAModelinPhysiotherapyDocument5 pagesReeducationSensorimotor PrinciplesandAModelinPhysiotherapyayuNo ratings yet
- How To Take Your TimeDocument3 pagesHow To Take Your TimePhương Hân TrầnNo ratings yet
- Donald Ingber. The Architecture of LifeDocument10 pagesDonald Ingber. The Architecture of LifeGreg Hill100% (1)
- Research Through DESIGN Through Research - Wolfgang JonasDocument8 pagesResearch Through DESIGN Through Research - Wolfgang Jonasis03lcmNo ratings yet
- Merleau-Ponty, Philosophy of LanguageDocument7 pagesMerleau-Ponty, Philosophy of LanguageakansrlNo ratings yet
- Eft Vets Study PDFDocument13 pagesEft Vets Study PDFKing GeorgeNo ratings yet
- Merleau-Ponty A Phenomenological Philoso PDFDocument34 pagesMerleau-Ponty A Phenomenological Philoso PDFThangneihsialNo ratings yet
- Habit and Situational Typification in Husserltional Typification in HusserlDocument20 pagesHabit and Situational Typification in Husserltional Typification in HusserlpcavicchNo ratings yet
- 1 Phenomenology and Embodied CognitionDocument10 pages1 Phenomenology and Embodied CognitionKiran GorkiNo ratings yet
- Kammers Et Al 2006 NeuropsychologiaDocument7 pagesKammers Et Al 2006 NeuropsychologiaAndreia SilvaNo ratings yet
- Contract Law Assignment: I. Certainty, Completeness and The Intention To Create Legal RelationsDocument9 pagesContract Law Assignment: I. Certainty, Completeness and The Intention To Create Legal RelationsPhilip Reynor Jr.100% (1)
- Super and Anonymised InjunctionsDocument12 pagesSuper and Anonymised InjunctionsPhilip Reynor Jr.No ratings yet
- Hard Cases Make Bad Law - An Examination of R V Caldwell (1982)Document11 pagesHard Cases Make Bad Law - An Examination of R V Caldwell (1982)Philip Reynor Jr.No ratings yet
- Haugeland - Mind Embodied and EmbeddedDocument16 pagesHaugeland - Mind Embodied and EmbeddedPhilip Reynor Jr.100% (2)
- Gallagher - Self-Reference and SchizophreniaDocument42 pagesGallagher - Self-Reference and SchizophreniaPhilip Reynor Jr.No ratings yet
- Husserl - The Idea of A Philosophical Culture.Document10 pagesHusserl - The Idea of A Philosophical Culture.Philip Reynor Jr.No ratings yet
- Zahavi 1994 - Husserl's Phenomenology of The BodyDocument12 pagesZahavi 1994 - Husserl's Phenomenology of The BodyPhilip Reynor Jr.No ratings yet
- Notion of The Natural Attitude and The Shift To Transcendental PhenomenologyDocument10 pagesNotion of The Natural Attitude and The Shift To Transcendental PhenomenologyMihail EvansNo ratings yet
- Husserl's Critique of NaturalismDocument25 pagesHusserl's Critique of NaturalismDavid JonesNo ratings yet
- Husserl - On The Phenomenology of Consciousness of Internal TimeDocument234 pagesHusserl - On The Phenomenology of Consciousness of Internal TimePhilip Reynor Jr.100% (13)
- Husserl - Ideas IIDocument229 pagesHusserl - Ideas IIPhilip Reynor Jr.100% (1)
- The World As Will: On Schopenhauer's Central ThesisDocument9 pagesThe World As Will: On Schopenhauer's Central ThesisPhilip Reynor Jr.No ratings yet
- AD 317 - Use of Integral Crossheads in Skew Highway BridgesDocument2 pagesAD 317 - Use of Integral Crossheads in Skew Highway Bridgessymon ellimacNo ratings yet
- 4TH Quarter Exam English IvDocument3 pages4TH Quarter Exam English IvTeacher ShairaNo ratings yet
- A Watch by Peter Henlein in LondonDocument13 pagesA Watch by Peter Henlein in LondonbahchovanskiNo ratings yet
- The Thorax and LungsDocument3 pagesThe Thorax and LungsAdellia PuspitasariNo ratings yet
- GRADES 1-12 Daily Lesson LOG School Grade Level Teacher Learning Area Teaching Dates and Time QuarterDocument2 pagesGRADES 1-12 Daily Lesson LOG School Grade Level Teacher Learning Area Teaching Dates and Time QuarterZyreane FernandezNo ratings yet
- HCM Cloud - Global HR - New Hire and Manage ChangesDocument53 pagesHCM Cloud - Global HR - New Hire and Manage ChangesRAM SNo ratings yet
- Fao 2016 The State of Food and Agriculture PDFDocument194 pagesFao 2016 The State of Food and Agriculture PDFYenny Rodriguez100% (1)
- UML IntroductionDocument120 pagesUML IntroductionjamesNo ratings yet
- KMU Vs Garcia - Case DigestDocument1 pageKMU Vs Garcia - Case DigestJEANDEE FEI LEONORNo ratings yet
- KNPCC-13 Nit KNPCC 13Document10 pagesKNPCC-13 Nit KNPCC 13Shubh ShuklaNo ratings yet
- C++ FunctionsDocument96 pagesC++ FunctionsDesadaNo ratings yet
- Gigabyte GA-H81M-S2VDocument32 pagesGigabyte GA-H81M-S2VDan Lucian PopaNo ratings yet
- Dynamic Presentations Feedback FormsDocument15 pagesDynamic Presentations Feedback FormsAnastasiia DrapakNo ratings yet
- Revuto Token SaleDocument1 pageRevuto Token Salekiranmai27No ratings yet
- Binary and Hexadecimal Number SystemDocument4 pagesBinary and Hexadecimal Number Systemkaran007_m100% (3)
- 32'' LT662VDocument11 pages32'' LT662VSathishKumar VenkatesanNo ratings yet
- CV JanetDocument2 pagesCV JanetGuar GumNo ratings yet
- Are Diet Supplements The Whey Forward?Document7 pagesAre Diet Supplements The Whey Forward?Jason Darrell100% (1)
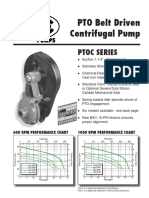
- Ptoc 03-13Document4 pagesPtoc 03-13Matias Contreras KöbrichNo ratings yet
- Husham Issa Al-SaleemDocument21 pagesHusham Issa Al-SaleemlmiitobnykhpvdwuzyNo ratings yet
- Cambridge IGCSE™: Additional Mathematics 0606/13Document9 pagesCambridge IGCSE™: Additional Mathematics 0606/13Rishwin Singh Sinda a/l Karamjeet SinghNo ratings yet