You might also like
- Benefit of Partial Right-Bilateral Internal Thoracic Artery Harvesting in Patients at Risk of Sternal Wound ComplicationsDocument5 pagesBenefit of Partial Right-Bilateral Internal Thoracic Artery Harvesting in Patients at Risk of Sternal Wound Complicationsfluid_man_brazilNo ratings yet
- Tumor Necrosis Factor Alpha Influences The Inflammatory Response After Coronary SurgeryDocument6 pagesTumor Necrosis Factor Alpha Influences The Inflammatory Response After Coronary Surgeryfluid_man_brazilNo ratings yet
- Effects of Papaverine and Glycerilnitrate-Verapamil Solution As Topical and Intraluminal Vasodilators For Internal Thoracic ArteryDocument5 pagesEffects of Papaverine and Glycerilnitrate-Verapamil Solution As Topical and Intraluminal Vasodilators For Internal Thoracic Arteryfluid_man_brazilNo ratings yet
- Attracting Outstanding Students (Premedical and Medical) To A Career in Cardiothoracic SurgeryDocument3 pagesAttracting Outstanding Students (Premedical and Medical) To A Career in Cardiothoracic Surgeryfluid_man_brazilNo ratings yet
- Comparative Effects of Tolazoline and Nitroprusside On Human Isolated Radial ArteryDocument7 pagesComparative Effects of Tolazoline and Nitroprusside On Human Isolated Radial Arteryfluid_man_brazilNo ratings yet
- Splanchnic Organ Injury During Coronary Surgery With or Without Cardiopulmonary Bypass: A Randomized, Controlled TrialDocument7 pagesSplanchnic Organ Injury During Coronary Surgery With or Without Cardiopulmonary Bypass: A Randomized, Controlled Trialfluid_man_brazilNo ratings yet
- Physicians Assistants in Cardiothoracic Surgery: A 30-Year Experience in A University CenterDocument6 pagesPhysicians Assistants in Cardiothoracic Surgery: A 30-Year Experience in A University Centerfluid_man_brazilNo ratings yet
- Wrapping of The Left Internal Thoracic Artery With An Expanded Polytetrafluoroethylene MembraneDocument3 pagesWrapping of The Left Internal Thoracic Artery With An Expanded Polytetrafluoroethylene Membranefluid_man_brazilNo ratings yet
- Aprotinin Shows Both Hemostatic and Antithrombotic Effects During Off-Pump Coronary Artery Bypass GraftingDocument8 pagesAprotinin Shows Both Hemostatic and Antithrombotic Effects During Off-Pump Coronary Artery Bypass Graftingfluid_man_brazilNo ratings yet
- (Radial String Sign) PDFDocument8 pages(Radial String Sign) PDFfluid_man_brazilNo ratings yet
- Myocardial Thievery: The Coronary-Subclavian Steal SyndromeDocument7 pagesMyocardial Thievery: The Coronary-Subclavian Steal Syndromefluid_man_brazilNo ratings yet
- Off-Pump Myocardial Revascularization: Critical Analysis of 23 Years' Experience in 3,866 PatientsDocument5 pagesOff-Pump Myocardial Revascularization: Critical Analysis of 23 Years' Experience in 3,866 Patientsfluid_man_brazilNo ratings yet
- Images - Multiple Penetrating Aortic UlcersDocument1 pageImages - Multiple Penetrating Aortic Ulcersfluid_man_brazilNo ratings yet
- Personal Communication - A Piece of Glass in The HeartDocument2 pagesPersonal Communication - A Piece of Glass in The Heartfluid_man_brazilNo ratings yet
- Intraoperative and Postoperative Evaluation of Cavitation in Mechanical Heart Valve PatientsDocument8 pagesIntraoperative and Postoperative Evaluation of Cavitation in Mechanical Heart Valve Patientsfluid_man_brazilNo ratings yet
- Long-Term Neurocognitive Function After Mechanical Aortic Valve ReplacementDocument5 pagesLong-Term Neurocognitive Function After Mechanical Aortic Valve Replacementfluid_man_brazilNo ratings yet
- Coapsys Mitral Annuloplasty For Chronic Functional Ischemic Mitral Regurgitation: 1-Year ResultsDocument5 pagesCoapsys Mitral Annuloplasty For Chronic Functional Ischemic Mitral Regurgitation: 1-Year Resultsfluid_man_brazilNo ratings yet
- Coronary Artery Revascularization After Chest Wall Reconstruction With Rectus Abdominis Myocutaneous FlapDocument4 pagesCoronary Artery Revascularization After Chest Wall Reconstruction With Rectus Abdominis Myocutaneous Flapfluid_man_brazilNo ratings yet
- How To Do It - Alternative Bi-Pectoral Muscle Flaps For Postoperative Sternotomy MediastinitisDocument2 pagesHow To Do It - Alternative Bi-Pectoral Muscle Flaps For Postoperative Sternotomy Mediastinitisfluid_man_brazilNo ratings yet
- Three-Dimensional Demonstration of The Collateral Circulation To The Artery of Adamkiewicz With 16-Row Multislice Computed TomographyDocument1 pageThree-Dimensional Demonstration of The Collateral Circulation To The Artery of Adamkiewicz With 16-Row Multislice Computed Tomographyfluid_man_brazilNo ratings yet
- The Society of Thoracic Surgeons/American Association For Thoracic Surgery Off-Pump Training ProgramDocument3 pagesThe Society of Thoracic Surgeons/American Association For Thoracic Surgery Off-Pump Training Programfluid_man_brazilNo ratings yet
- Effect of Aprotinin and Recombinant Variants On Platelet Protease-Activated Receptor 1 ActivationDocument6 pagesEffect of Aprotinin and Recombinant Variants On Platelet Protease-Activated Receptor 1 Activationfluid_man_brazilNo ratings yet
- Early Postoperative Anticoagulation After Mechanical Valve Replacement: A Systematic ReviewDocument12 pagesEarly Postoperative Anticoagulation After Mechanical Valve Replacement: A Systematic Reviewfluid_man_brazilNo ratings yet
- Effect of Aprotinin and Recombinant Variants On Platelet Protease-Activated Receptor 1 ActivationDocument6 pagesEffect of Aprotinin and Recombinant Variants On Platelet Protease-Activated Receptor 1 Activationfluid_man_brazilNo ratings yet
- Portable Coronary Active Perfusion System For Off-Pump Coronary Artery Bypass GraftingDocument5 pagesPortable Coronary Active Perfusion System For Off-Pump Coronary Artery Bypass Graftingfluid_man_brazilNo ratings yet
- Invited Commentary - New Technology - New Perfusion System For Opcabg (Koshida Et Al)Document2 pagesInvited Commentary - New Technology - New Perfusion System For Opcabg (Koshida Et Al)fluid_man_brazilNo ratings yet
- Invited Commentary - Preoperative WBC Link To Cabg Outcome (Newall Et Al)Document2 pagesInvited Commentary - Preoperative WBC Link To Cabg Outcome (Newall Et Al)fluid_man_brazilNo ratings yet
- Prevention of Postoperative Pericardial Adhesions With A Novel Regenerative Collagen SheetDocument8 pagesPrevention of Postoperative Pericardial Adhesions With A Novel Regenerative Collagen Sheetfluid_man_brazilNo ratings yet
- Invited Commentary - Aprotinin and Recombinant Variants (Day Et Al)Document1 pageInvited Commentary - Aprotinin and Recombinant Variants (Day Et Al)fluid_man_brazilNo ratings yet
- Invited Commentary - No Volume-Outcome Relationship For Opcabg (Plomondon Et Al)Document2 pagesInvited Commentary - No Volume-Outcome Relationship For Opcabg (Plomondon Et Al)fluid_man_brazilNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Sip InformationDocument111 pagesSip InformationakashNo ratings yet
- Far North Thrive Expo 2015 BookletDocument20 pagesFar North Thrive Expo 2015 BookletNicola YoungNo ratings yet
- CBT therapy overview: strengths, sessions, evidenceDocument1 pageCBT therapy overview: strengths, sessions, evidencezulkaberNo ratings yet
- Reducing AgeismDocument2 pagesReducing AgeismAntónio LealNo ratings yet
- CHCCOM005 Student Assessment Booklet (ID 98950)Document79 pagesCHCCOM005 Student Assessment Booklet (ID 98950)Hardeek Mota25% (20)
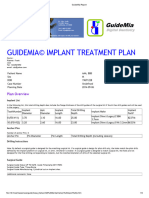
- GuideMia Sample Report - EnglishDocument9 pagesGuideMia Sample Report - Englishzhiao liuNo ratings yet
- Ruptured Globe Involving Cornea Dictation GuideDocument2 pagesRuptured Globe Involving Cornea Dictation GuideErik Anderson MDNo ratings yet
- Acutrak2 Radial Head Case StudyDocument2 pagesAcutrak2 Radial Head Case StudyDinesh KumarNo ratings yet
- Chapter 6 - Adipose TissueDocument13 pagesChapter 6 - Adipose TissueREMAN ALINGASANo ratings yet
- Abc of Burns: Kanwal Khan Lecturer ZCPTDocument35 pagesAbc of Burns: Kanwal Khan Lecturer ZCPTKanwal KhanNo ratings yet
- Product Lifecycle ManagementDocument27 pagesProduct Lifecycle ManagementDeepanshu ChawlaNo ratings yet
- Blue Plains Plant Brochure PDFDocument7 pagesBlue Plains Plant Brochure PDFAfzal AhmadNo ratings yet
- Failure To ThriveDocument3 pagesFailure To Thriveibbs91No ratings yet
- Safety Data Sheet Picric Acid (Alcoholic)Document14 pagesSafety Data Sheet Picric Acid (Alcoholic)tarek aneesNo ratings yet
- C11 - Study 1Document6 pagesC11 - Study 1zeeshan78No ratings yet
- Body PlethysmographyDocument52 pagesBody PlethysmographyppgpcsNo ratings yet
- Rusty Moore Visual Impact For WomenDocument34 pagesRusty Moore Visual Impact For Womenchrisie00757% (7)
- Shean19 VaPID RefthroughGeneBankDocument8 pagesShean19 VaPID RefthroughGeneBankAnh H NguyenNo ratings yet
- WIC Authorized Food List: Shopping GuideDocument17 pagesWIC Authorized Food List: Shopping GuideGanda PrajaNo ratings yet
- Echo - Medical Supplies and Equipment For Primary Health CareDocument192 pagesEcho - Medical Supplies and Equipment For Primary Health CareKing Solomon CatralNo ratings yet
- Mathematics in The Modern World: Introduction To LogicDocument17 pagesMathematics in The Modern World: Introduction To LogicOnecho Angelo Gabinete0% (1)
- Forced Abortions ExposedDocument26 pagesForced Abortions Exposedesorenson1No ratings yet
- Capstone SolutionDocument1 pageCapstone Solutiondave magcawasNo ratings yet
- How To Know If U Need Ortho TTDocument3 pagesHow To Know If U Need Ortho TTSubhajit SahaNo ratings yet
- Concure WB309 MSDSDocument7 pagesConcure WB309 MSDSAmeer KhanNo ratings yet
- Cutaneous Manifestations of Juvenile Onset Lupus Erythematosus: A Clinical StudyDocument5 pagesCutaneous Manifestations of Juvenile Onset Lupus Erythematosus: A Clinical StudyMaya SusantiNo ratings yet
- CUSTOM - LETTER - RPT - Custom Tailored Email - REV C - v5Document2 pagesCUSTOM - LETTER - RPT - Custom Tailored Email - REV C - v5Aaron De VeraNo ratings yet
- 09 ICSH Review of The Measurement of The ESR PDFDocument8 pages09 ICSH Review of The Measurement of The ESR PDFMuslim Majlis UojNo ratings yet
- Optima Restore Rate Card Inclusive of Service TaxDocument2 pagesOptima Restore Rate Card Inclusive of Service Taxmksnake77No ratings yet
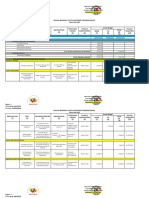
- ABYIP-2023 TemplateDocument3 pagesABYIP-2023 Templatejomar88% (26)