You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Protocolo TACODocument33 pagesProtocolo TACOsamnachoNo ratings yet
- Toxoplasmosis and Suicide: It's Probably Not The Cats Causing Danish Women To Kill Themselves.Document1 pageToxoplasmosis and Suicide: It's Probably Not The Cats Causing Danish Women To Kill Themselves.samnachoNo ratings yet
- Chanel No. 5: A Brain Parasite May Be The Secret To The Famous Perfume PDFDocument1 pageChanel No. 5: A Brain Parasite May Be The Secret To The Famous Perfume PDFsamnachoNo ratings yet
- Getting Started With Song Specific PatchesDocument1 pageGetting Started With Song Specific PatchessamnachoNo ratings yet
- Could A Brain Parasite Found in Cats Help Soccer Teams Win at The World Cup?Document1 pageCould A Brain Parasite Found in Cats Help Soccer Teams Win at The World Cup?samnachoNo ratings yet
- A Womans Right To Choose - Designation of Fetal Tissue DoneesDocument25 pagesA Womans Right To Choose - Designation of Fetal Tissue DoneessamnachoNo ratings yet
- Cap 4Document9 pagesCap 4samnachoNo ratings yet
- Reassessing The Role of Astrocytes in Ammonia NeurotoxicityDocument3 pagesReassessing The Role of Astrocytes in Ammonia NeurotoxicitysamnachoNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Diabetes Reversal by Plant Based Diet Dr. BiswaroopDocument18 pagesDiabetes Reversal by Plant Based Diet Dr. BiswaroopvhirNo ratings yet
- Models For Predicting Type 1 Diabetes in Siblings of Affected ChildrenDocument6 pagesModels For Predicting Type 1 Diabetes in Siblings of Affected ChildrenRatu TanpanyaNo ratings yet
- Endo NclexDocument17 pagesEndo Nclexal-obinay shereenNo ratings yet
- C Peptide AeedecDocument11 pagesC Peptide AeedecAl-rawi NatheerNo ratings yet
- Diabetes and Hearing Loss (Pamela Parker MD)Document2 pagesDiabetes and Hearing Loss (Pamela Parker MD)Sartika Rizky HapsariNo ratings yet
- RN Review QuestionDocument7 pagesRN Review QuestionFaith Levi Alecha AlferezNo ratings yet
- HTTP Healthmedicinet Com II 2013 9 PDFDocument223 pagesHTTP Healthmedicinet Com II 2013 9 PDFtuni santeNo ratings yet
- Amiat Risk For Diabetes?: Type 2Document23 pagesAmiat Risk For Diabetes?: Type 2apriraNo ratings yet
- Diabetes Mellitus Type 1: Medical Ethics IiiDocument16 pagesDiabetes Mellitus Type 1: Medical Ethics IiiGiane DavidNo ratings yet
- Quotes On Vaccines by Health Care ExpertsDocument29 pagesQuotes On Vaccines by Health Care ExpertsM. R. WildeNo ratings yet
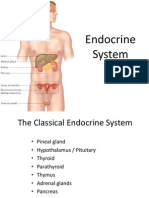
- Endocrine SystemDocument96 pagesEndocrine SystemSandhya Kakkar100% (3)
- Diagnosis and Treatment of Diabetes Mellitus in Chronic PancreatitisDocument7 pagesDiagnosis and Treatment of Diabetes Mellitus in Chronic PancreatitisFarid TaufiqNo ratings yet
- Concept PaperDocument12 pagesConcept Paperjlventigan100% (1)
- 101 Black Seed Oil BenefitsDocument15 pages101 Black Seed Oil BenefitsTAMBAKI EDMOND100% (4)
- E61 PDFDocument39 pagesE61 PDFElizabeth SniderNo ratings yet
- Pink Panther - Diabetes Management - Chapter 22Document16 pagesPink Panther - Diabetes Management - Chapter 22jennmoyerNo ratings yet
- Research Paper DiabetesDocument8 pagesResearch Paper Diabetesapi-359023534No ratings yet
- 395 Pharmacy GuideDocument25 pages395 Pharmacy GuideSAEEDAAHMERNo ratings yet
- C PeptideDocument8 pagesC Peptideapril babyNo ratings yet
- American College of Sports MedicineDocument62 pagesAmerican College of Sports MedicineLuiz CarvalhoNo ratings yet
- Diabetes ProjectDocument12 pagesDiabetes ProjectrollyNo ratings yet
- Dental Diabetes ManagementDocument30 pagesDental Diabetes ManagementChitrang KolawaleNo ratings yet
- Dietary Management of GI DiseasesDocument12 pagesDietary Management of GI DiseasesMiguel Cuevas DolotNo ratings yet
- Herbal Drugs For Diabetes CureDocument7 pagesHerbal Drugs For Diabetes CurenrrkrNo ratings yet
- Hyponidd Combination Rationale 2013 REV1Document26 pagesHyponidd Combination Rationale 2013 REV1Mitzi MitchellNo ratings yet
- Diabetes & Stem Cell - Poster.Document1 pageDiabetes & Stem Cell - Poster.Cardio VascularNo ratings yet
- Diabetes Mellitus IIDocument20 pagesDiabetes Mellitus IIMa R Dy100% (1)
- Case Presentation On Diabetic KetoacidosisDocument50 pagesCase Presentation On Diabetic KetoacidosisJoana Marie Gantuangco-MaglinteNo ratings yet
- Research Article: Antidiabetic Activity of Ethanolic Extract of Hyperglycaemic RatsDocument6 pagesResearch Article: Antidiabetic Activity of Ethanolic Extract of Hyperglycaemic RatsUmmu Ghodah ZurrahmiNo ratings yet
- Autoimmune Disease - Why and Where It OccursDocument7 pagesAutoimmune Disease - Why and Where It OccursdNo ratings yet