You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5811)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Original PDF Medical Terminology For Health Care Professionals A Word Building Approach 9th PDFDocument42 pagesOriginal PDF Medical Terminology For Health Care Professionals A Word Building Approach 9th PDFmegan.soffel782100% (41)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Registrasi Izin Edar ALKES Elektromedik Impor PDFDocument224 pagesRegistrasi Izin Edar ALKES Elektromedik Impor PDFraziabikini67% (3)
- Disability Report-Adult-Form Ssa-3368-Bk Read All of This Information Before You Begin Completing This Form If You Need HelpDocument81 pagesDisability Report-Adult-Form Ssa-3368-Bk Read All of This Information Before You Begin Completing This Form If You Need HelpHenry Jacob Baker JrNo ratings yet
- Lesson Plan Human Eye Class XDocument11 pagesLesson Plan Human Eye Class Xminakshi tiwari70% (10)
- Basic of AccupressureDocument48 pagesBasic of AccupressureRavikumarrd Ravi100% (2)
- Qeh Ambulatory Care ServicesDocument2 pagesQeh Ambulatory Care Servicesrobinmilton1998No ratings yet
- Rare Congenital Genitourinary AnomaliesDocument27 pagesRare Congenital Genitourinary Anomaliesد. محمد عبد الباقي فهميNo ratings yet
- AMA Assignment 5Document2 pagesAMA Assignment 5Ali AmarNo ratings yet
- 403-Guidelines Blood Collection Volumes and Frequency - Sept 2017 0Document7 pages403-Guidelines Blood Collection Volumes and Frequency - Sept 2017 0Diana OlvediNo ratings yet
- Nur 101 Data Base 1Document23 pagesNur 101 Data Base 1api-337919180No ratings yet
- Oral and Maxillofacial Radiology: Oral Surgery Oral Medicine Oral PathologyDocument6 pagesOral and Maxillofacial Radiology: Oral Surgery Oral Medicine Oral PathologynisaNo ratings yet
- Practical Class 1Document16 pagesPractical Class 1Chahinez HabibNo ratings yet
- Tenses Paper PDFDocument11 pagesTenses Paper PDFDewiandikaNo ratings yet
- Apheresis: For PlasmaDocument6 pagesApheresis: For PlasmaKarla Chariz Fernandez BayagNo ratings yet
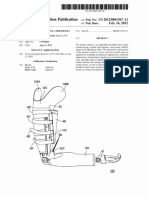
- Us 20120041567Document28 pagesUs 20120041567Anugrah YudhaNo ratings yet
- NHS Highland Wound Management Guidelines and Formulary PDFDocument91 pagesNHS Highland Wound Management Guidelines and Formulary PDFubayyumr100% (1)
- Hypertension: Dr. Isbandiyah, SPPD FK UmmDocument41 pagesHypertension: Dr. Isbandiyah, SPPD FK UmmSemestaNo ratings yet
- Development of A Topical Gel Containing A Dipeptidyl Peptidase-4 Inhibitor For Wound Healing ApplicationsDocument15 pagesDevelopment of A Topical Gel Containing A Dipeptidyl Peptidase-4 Inhibitor For Wound Healing ApplicationsGlobal Research and Development ServicesNo ratings yet
- Visual Pathway DR FKDocument36 pagesVisual Pathway DR FKamaliaramadhani100% (1)
- Psychosocial IntegrityDocument3 pagesPsychosocial IntegrityRojannie SalenNo ratings yet
- Icd 10Document170 pagesIcd 10Silverius Seantoni SabellaNo ratings yet
- Intubasi - Dr. Hasan SpAnDocument42 pagesIntubasi - Dr. Hasan SpAnAlessia Wyneini TirzaNo ratings yet
- Parental Alienation, DSM-V, and ICD-11Document113 pagesParental Alienation, DSM-V, and ICD-11Talia Schwartz67% (6)
- TiredDocument1 pageTiredNelson AvilaNo ratings yet
- 16 Preovulatory Stasis Dystocia in Oviparous Lizards PDFDocument4 pages16 Preovulatory Stasis Dystocia in Oviparous Lizards PDFRizza SainTrow VeiroNo ratings yet
- Pediatric Ambulatory PDFDocument20 pagesPediatric Ambulatory PDFjavajavuNo ratings yet
- Fulminant Hepatic FailureDocument53 pagesFulminant Hepatic FailureAR KarthickNo ratings yet
- TBI Research DirectoryDocument330 pagesTBI Research Directorybradfordmccall1No ratings yet
- Nodular Rheumatoid Arthritis Resembling Gout: Katrina Chakradeo, Katie Buzacott, Muriel SodenDocument2 pagesNodular Rheumatoid Arthritis Resembling Gout: Katrina Chakradeo, Katie Buzacott, Muriel SodenrhizkyNo ratings yet