You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Podiatry Institute ManualDocument301 pagesPodiatry Institute ManualTyler Lawrence Coye100% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Test Bank For Medical Terminology For Health Care Professionals 9th Edition Jane RiceDocument38 pagesTest Bank For Medical Terminology For Health Care Professionals 9th Edition Jane Ricemichellehermanjbokgyqtfs100% (23)
- Gerbert Text Study GuideDocument54 pagesGerbert Text Study GuideAndrea RaeNo ratings yet
- The Renaissance of The Greek Ideal - Emily Diana Watts (1867-1968)Document374 pagesThe Renaissance of The Greek Ideal - Emily Diana Watts (1867-1968)nahualpa646No ratings yet
- Thai Foot Reflexology for Health A Practical Manual คู่มือนวดเท้ากดจุดเพื่อสุขภาพDocument25 pagesThai Foot Reflexology for Health A Practical Manual คู่มือนวดเท้ากดจุดเพื่อสุขภาพศาสตรา คำมุลตรี100% (2)
- Typhoid Fever InternaDocument14 pagesTyphoid Fever InternaMira Arlita RahmawatiNo ratings yet
- Pamj 23 197Document9 pagesPamj 23 197ratihNo ratings yet
- JadNew PrintDocument3 pagesJadNew PrintratihNo ratings yet
- HyperemesisDocument8 pagesHyperemesisjayyidfifah92No ratings yet
- Jurnal PDFDocument9 pagesJurnal PDFratihNo ratings yet
- Use of Neutrophil Count in Early Diagnosis and Risk Stratification of AMIDocument9 pagesUse of Neutrophil Count in Early Diagnosis and Risk Stratification of AMIratihNo ratings yet
- Cover Journal ReadingDocument2 pagesCover Journal ReadingVera Utami DewiNo ratings yet
- Combined Nivolumab and Ipilimumab or Monotherapy in Untreated MelanomaDocument12 pagesCombined Nivolumab and Ipilimumab or Monotherapy in Untreated MelanomaratihNo ratings yet
- Jurnal Anes1Document5 pagesJurnal Anes1ratihNo ratings yet
- Frequencies: Lampiran 3Document6 pagesFrequencies: Lampiran 3ratihNo ratings yet
- COVERDocument2 pagesCOVERratihNo ratings yet
- Jurnal Anes1Document5 pagesJurnal Anes1ratihNo ratings yet
- Association of Contact Lens-Related Alle PDFDocument6 pagesAssociation of Contact Lens-Related Alle PDFratihNo ratings yet
- Cotrimoxazole Prophylaxis and Tuberculosis Risk Among People Living With HIVDocument5 pagesCotrimoxazole Prophylaxis and Tuberculosis Risk Among People Living With HIVTitis MeyliawatiNo ratings yet
- Anestesi Pasien Pediatrik: Pull Trough Hirschsprung'S DiseaseDocument2 pagesAnestesi Pasien Pediatrik: Pull Trough Hirschsprung'S DiseaseratihNo ratings yet
- Weight-For-Length BOYS: Birth To 2 Years (Z-Scores)Document1 pageWeight-For-Length BOYS: Birth To 2 Years (Z-Scores)Malisa LukmanNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaNia FitriyaniNo ratings yet
- Weight-For-Length BOYS: Birth To 2 Years (Z-Scores)Document1 pageWeight-For-Length BOYS: Birth To 2 Years (Z-Scores)Malisa LukmanNo ratings yet
- Follow Up Interna ALDocument2 pagesFollow Up Interna ALratihNo ratings yet
- DwewdDocument3 pagesDwewdratihNo ratings yet
- Q2 Nail Care Services 9 Module 3 W3 4 PDFDocument20 pagesQ2 Nail Care Services 9 Module 3 W3 4 PDFkrinessa erika m. de chavezNo ratings yet
- 2009 - Bosch Osteotomy Vs Scarf in Hallux ValgusDocument10 pages2009 - Bosch Osteotomy Vs Scarf in Hallux ValgusMiguel Angel Palacios FloresNo ratings yet
- PPL 2010 CatalogueDocument107 pagesPPL 2010 CatalogueOMF PublicityNo ratings yet
- Touch The Toes Test.0812 PDFDocument4 pagesTouch The Toes Test.0812 PDFEliza MagopetNo ratings yet
- The Manufacture of Boots and Shoes 1000747941Document321 pagesThe Manufacture of Boots and Shoes 1000747941adiseif100% (3)
- Ch. Neurology (7th Ed.)Document1,506 pagesCh. Neurology (7th Ed.)Giorgos KarvelasNo ratings yet
- 24.amputations of The Foot and AnkleDocument29 pages24.amputations of The Foot and AnklesteoeviciNo ratings yet
- ParonychiaDocument1 pageParonychiaFaishal HusniNo ratings yet
- Rotational Flap Closure of 1st and 5nth Met HeadDocument8 pagesRotational Flap Closure of 1st and 5nth Met HeadleahbayNo ratings yet
- Local Anesthesia Techniques PDFDocument12 pagesLocal Anesthesia Techniques PDFhalimNo ratings yet
- Ergonomics in Apparel IndustryDocument23 pagesErgonomics in Apparel IndustryAnkit SinghNo ratings yet
- Reflexology BibleDocument84 pagesReflexology BibleenyaNo ratings yet
- Rivero 1991. New Ecuadorean Colostethus (Amphibia, Dendrobatidae) in The Collection of The National Museum of Natural History, Smithsonian InstitutionDocument16 pagesRivero 1991. New Ecuadorean Colostethus (Amphibia, Dendrobatidae) in The Collection of The National Museum of Natural History, Smithsonian InstitutionNicole AcosVas0% (1)
- Diabetes Foot Screen: - Can't Feel The 5.07 FilamentDocument4 pagesDiabetes Foot Screen: - Can't Feel The 5.07 FilamentSteve ChipmanNo ratings yet
- Opposite Fingers and ToesDocument1 pageOpposite Fingers and Toescchlomas4269100% (6)
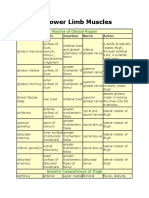
- Lower Limb MusclesDocument8 pagesLower Limb Musclesbilal_kmu020% (1)
- Hallux ValgusDocument16 pagesHallux ValgusucssNo ratings yet
- Hallux VarusDocument12 pagesHallux VarusZam PamateNo ratings yet
- Normal Foot and Ankle Radiographic Angles, Measurements, and Reference PointsDocument8 pagesNormal Foot and Ankle Radiographic Angles, Measurements, and Reference PointsCinthya BorgesNo ratings yet
- Bunion Surgery - Foot - Surgery - What We Treat - Physio - Co.ukDocument35 pagesBunion Surgery - Foot - Surgery - What We Treat - Physio - Co.ukvaishnaviNo ratings yet
- KINESIOLOGY - Carmina Cortez, MD - September 27, 2017Document9 pagesKINESIOLOGY - Carmina Cortez, MD - September 27, 2017Johann Sebastian CruzNo ratings yet
- Lesser Metatarsal Osteotomy Complications: Lowell S. Weil and Erin E. KleinDocument9 pagesLesser Metatarsal Osteotomy Complications: Lowell S. Weil and Erin E. KleinAntonio FloresNo ratings yet
- Review - Presby Residency ManualDocument400 pagesReview - Presby Residency ManualSneha SutharNo ratings yet
- Longitudinal Epiphyseal Bracket of The First Metatarsal Bone: Three Case Reports and A Review of The LiteratureDocument7 pagesLongitudinal Epiphyseal Bracket of The First Metatarsal Bone: Three Case Reports and A Review of The LiteraturebaoNo ratings yet
- Examination of Orthopedic Athletic Injuries 4th Edition Starkey Test BankDocument11 pagesExamination of Orthopedic Athletic Injuries 4th Edition Starkey Test Bankhungden8pne100% (37)