You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- GI Motility FunctionsDocument10 pagesGI Motility FunctionsSiva RajeshwarNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Ca MammaeDocument43 pagesCa MammaeAnonymous F0eeZBMKNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- IBD MedicationDocument19 pagesIBD MedicationTheghanNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Klinghardt - A Unique HealerDocument30 pagesKlinghardt - A Unique HealerAna Simionov100% (2)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
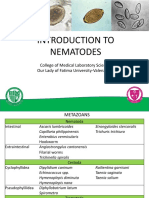
- Introduction To Nematodes: College of Medical Laboratory Science Our Lady of Fatima University-ValenzuelaDocument29 pagesIntroduction To Nematodes: College of Medical Laboratory Science Our Lady of Fatima University-ValenzuelaMichNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Draft Toxicological Profile For Fluorine, Hydrogen Fluoride, and FluoridesDocument354 pagesDraft Toxicological Profile For Fluorine, Hydrogen Fluoride, and FluoridesMy-RavenNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Knowledge, Attitudes, and Practices Regarding Cervical Cancer and Screening Among Ethiopian Health Care WorkersDocument10 pagesKnowledge, Attitudes, and Practices Regarding Cervical Cancer and Screening Among Ethiopian Health Care WorkersSrideviRaviNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- 12-O-Tetradecanoylphorbol-13 - Acetate (TPA) Is Anti-Tumorigenic in Liver Cancer Cells Via Inhibiting YAP Through AMOT-srep44940Document11 pages12-O-Tetradecanoylphorbol-13 - Acetate (TPA) Is Anti-Tumorigenic in Liver Cancer Cells Via Inhibiting YAP Through AMOT-srep44940harrybzyNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- 20IB314 Bayer Corporation Vs Union of IndiaDocument12 pages20IB314 Bayer Corporation Vs Union of IndiaApoorv TyagiNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Chemical Peels in Aesthetic Dermatology - An Update 2009 PDFDocument12 pagesChemical Peels in Aesthetic Dermatology - An Update 2009 PDFjujuNo ratings yet
- ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( - Clinical Trial - (Publication Type) or - Clinical Trials - PubMed - NCBI45Document23 pages( ( ( ( ( ( ( ( ( ( ( ( ( ( ( - Clinical Trial - (Publication Type) or - Clinical Trials - PubMed - NCBI45Túlio Martins OliveiraNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Types of DoctorsDocument3 pagesTypes of DoctorsRenelyn Seno Llamazares100% (1)
- Daniel de Moulin. A Short History of Breast Cancer 1989Document133 pagesDaniel de Moulin. A Short History of Breast Cancer 1989aristotleargos100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Tuberculosis: Lifestyle (Smoking) Environment Age GenderDocument2 pagesTuberculosis: Lifestyle (Smoking) Environment Age GenderhannahleatanosornNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- MeningiomaDocument51 pagesMeningiomaarushijha2000No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Ficat and Arlet Staging of Avascular Necrosis of Femoral HeadDocument6 pagesFicat and Arlet Staging of Avascular Necrosis of Femoral HeadFernando Sugiarto0% (1)
- 3M Material Safety Data Sheet Electrical Moisture Sealant Pads (Ems Ii)Document7 pages3M Material Safety Data Sheet Electrical Moisture Sealant Pads (Ems Ii)danielliram993No ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Microwaves and Children at School - Barrie Trower TestimonyDocument23 pagesMicrowaves and Children at School - Barrie Trower Testimonyoinotnaissab100% (1)
- Related NCPDocument5 pagesRelated NCPLara GatbontonNo ratings yet
- Medicinal Chemistry: Review of Cucurbita Pepo (Pumpkin) Its Phytochemistry and PharmacologyDocument10 pagesMedicinal Chemistry: Review of Cucurbita Pepo (Pumpkin) Its Phytochemistry and PharmacologyfitriasarassNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 404 Veterinary Referral Hospital - BrochureDocument11 pages404 Veterinary Referral Hospital - BrochureJoanne FagnouNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Consent Transsphenoidal SurgeryDocument10 pagesConsent Transsphenoidal SurgeryAbhinav GuptaNo ratings yet
- Proceeding Book 28th Jakarta Diabates Meeting 2019Document19 pagesProceeding Book 28th Jakarta Diabates Meeting 2019David DwiputeraNo ratings yet
- MSDS Crude OilDocument6 pagesMSDS Crude OilFabio IkaczykNo ratings yet
- Make A Golden Mixture - The Strongest Antibiotic and Anti-Cancer Remedy (Guide For The Preparation and Method of Use)Document7 pagesMake A Golden Mixture - The Strongest Antibiotic and Anti-Cancer Remedy (Guide For The Preparation and Method of Use)CinNo ratings yet
- The Challenges of Nutritional Assessment in Geriatric Cancer Patients - UpdatedDocument31 pagesThe Challenges of Nutritional Assessment in Geriatric Cancer Patients - Updatedsuzana78m695No ratings yet
- 1358453842.3856hematology Question BankDocument182 pages1358453842.3856hematology Question BankKay BristolNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Amputation in Lower LimbsDocument35 pagesAmputation in Lower LimbsSamNo ratings yet
- ENT MCQsDocument13 pagesENT MCQsSheikha100% (2)
- HIV in PregnancyDocument28 pagesHIV in PregnancyRaja100% (1)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)