You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Freedman Vs MossDocument9 pagesFreedman Vs MossOras PhongNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Hypertension CASE STUDYDocument30 pagesHypertension CASE STUDYKaloy Kamao100% (7)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Physiologic Value of FoodDocument6 pagesPhysiologic Value of FoodMelanie Galedo100% (1)
- HEP-Hip Open Reduction Internal Fixation (ORIF) ExercisesDocument7 pagesHEP-Hip Open Reduction Internal Fixation (ORIF) ExercisesErlin IrawatiNo ratings yet
- A Case Study On AGE Part 3Document2 pagesA Case Study On AGE Part 3pangee489No ratings yet
- Trends and Innovations in Bakery Garcia EtalDocument14 pagesTrends and Innovations in Bakery Garcia Etaldaryll r gabutinNo ratings yet
- Hypothesis Testing - Analysis of Variance (ANOVA)Document14 pagesHypothesis Testing - Analysis of Variance (ANOVA)Kumar RajNo ratings yet
- Codex Stan 146 1985Document3 pagesCodex Stan 146 1985apostolidis83No ratings yet
- Module 1 Chemistry ChecklistDocument3 pagesModule 1 Chemistry ChecklistmojoaxfordNo ratings yet
- AquaPure Manual H0325600Document52 pagesAquaPure Manual H0325600gkoch75No ratings yet
- Carbon Compounds MCQ AnsDocument30 pagesCarbon Compounds MCQ AnsNg Swee Loong StevenNo ratings yet
- Spartan StrengthDocument3 pagesSpartan StrengthjmdentonNo ratings yet
- A Comparative Study of Topical Phenytoin Vs Conventional Wound Care in Diabetic UlcerDocument6 pagesA Comparative Study of Topical Phenytoin Vs Conventional Wound Care in Diabetic UlcerIOSRjournalNo ratings yet
- The Impact of Nutrition and Lifestyle Habits On The Health of Undergraduate University StudentsDocument5 pagesThe Impact of Nutrition and Lifestyle Habits On The Health of Undergraduate University StudentsAyanda KakazaNo ratings yet
- Reviewing The ChapterDocument4 pagesReviewing The ChapterMyca NealonNo ratings yet
- Saffola FittifyDocument11 pagesSaffola FittifyMahantesh mamadapurNo ratings yet
- Breastfeeding CounsellingDocument30 pagesBreastfeeding CounsellingHadeer Mahmoud AbuslimaNo ratings yet
- A Sample Expalined EssayDocument4 pagesA Sample Expalined Essaysarfaraz100% (1)
- What Is Diabetes, Its Types, Role of Insulin and Hypoglycemic Agents, Mode of Action, Side Effects, Pharmacodynamics and PharmacokineticsDocument9 pagesWhat Is Diabetes, Its Types, Role of Insulin and Hypoglycemic Agents, Mode of Action, Side Effects, Pharmacodynamics and PharmacokineticsIshaani GargNo ratings yet
- Research PosterDocument1 pageResearch Posterapi-739129968No ratings yet
- Micronutrient Program - Department of HealthDocument3 pagesMicronutrient Program - Department of HealthMelvin MarzanNo ratings yet
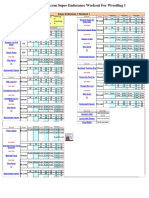
- Workout - Sheet - Wrestling Super Endurance 1 - 1477757519824 PDFDocument3 pagesWorkout - Sheet - Wrestling Super Endurance 1 - 1477757519824 PDFEduard-Marian RoventaNo ratings yet
- Exercise PrescriptionDocument87 pagesExercise PrescriptionDianne Faye ManabatNo ratings yet
- What Does My Hospital Diet MeanDocument6 pagesWhat Does My Hospital Diet Meanapi-455513786No ratings yet
- Reflection: (Physical Education 1)Document7 pagesReflection: (Physical Education 1)FaulknerMascardoNo ratings yet
- DENGUE Clinician GuideDocument8 pagesDENGUE Clinician GuideLuis Alfredo LaraNo ratings yet
- Athletic AdvantageDocument14 pagesAthletic AdvantagealibababuaNo ratings yet
- Concepts of Disease OccurrenceDocument24 pagesConcepts of Disease OccurrenceUma Mouna100% (1)
- Does Stress Influence Sleep Patterns Food Intake WDocument18 pagesDoes Stress Influence Sleep Patterns Food Intake Wpiyush thawraniNo ratings yet
- Palm T Case Study PresentationDocument18 pagesPalm T Case Study Presentationapi-305617091No ratings yet