You might also like
- Review of Literature: Multiple Osteogenic Sarcomata-Metastatic or Multicentric?Document9 pagesReview of Literature: Multiple Osteogenic Sarcomata-Metastatic or Multicentric?Srujan CherukuNo ratings yet
- Cancer - September 1965 - Mullins - Chondrosarcoma Following Synovial Chondromatosis A Case StudyDocument9 pagesCancer - September 1965 - Mullins - Chondrosarcoma Following Synovial Chondromatosis A Case StudyOvidiu MihailNo ratings yet
- Case Report on Chondrosarcoma of the Temporomandibular JointDocument9 pagesCase Report on Chondrosarcoma of the Temporomandibular JointCatalina Soler LioiNo ratings yet
- Jurnal 5Document3 pagesJurnal 5Centia PicalNo ratings yet
- Osteoblastoma A Spectrum of Presentation and TreatDocument10 pagesOsteoblastoma A Spectrum of Presentation and TreatmandetoperdiyuwanNo ratings yet
- ArnoldDocument5 pagesArnolddebby claudiNo ratings yet
- Painful Knee 2024 International Journal of Surgery Case ReportsDocument6 pagesPainful Knee 2024 International Journal of Surgery Case ReportsRonald QuezadaNo ratings yet
- 1.Case Report-A Rare Case of Inguinal Canal MalignancyDocument4 pages1.Case Report-A Rare Case of Inguinal Canal Malignancyunknownsince1986No ratings yet
- International Journal of Advances in Case ReportsDocument3 pagesInternational Journal of Advances in Case ReportsastritriNo ratings yet
- A Case of Malignant Pleural Mesothelioma With Metastasis To The OrbitDocument3 pagesA Case of Malignant Pleural Mesothelioma With Metastasis To The OrbitjamesyuNo ratings yet
- Extremity gossypiboma mimicking sarcoma: case report and reviewDocument7 pagesExtremity gossypiboma mimicking sarcoma: case report and reviewal qurtubi al andalusiNo ratings yet
- Case ReportDocument3 pagesCase Reportandrul556723No ratings yet
- Sakayama 2004Document4 pagesSakayama 2004al qurtubi al andalusiNo ratings yet
- Article in Press: Journal of Oral and Maxillofacial Surgery, Medicine, and PathologyDocument6 pagesArticle in Press: Journal of Oral and Maxillofacial Surgery, Medicine, and PathologyOMFS FKG UnimusNo ratings yet
- Mano 3Document5 pagesMano 3juanNo ratings yet
- ONCO 21 Desember 2020 Undiferentiated Pleomorfic Sarcoma Rev 1Document46 pagesONCO 21 Desember 2020 Undiferentiated Pleomorfic Sarcoma Rev 1ciptakarwanaNo ratings yet
- Schwarz, Richard - Medial Plantar ArteryDocument5 pagesSchwarz, Richard - Medial Plantar ArteryGrant DotulongNo ratings yet
- Ganglion Cyst of The Anterior Cruciate Ligament: A Case ReportDocument5 pagesGanglion Cyst of The Anterior Cruciate Ligament: A Case ReportDanni XNo ratings yet
- Unusual Presentation of Adamantinoma With Synchronous 2024 International JouDocument5 pagesUnusual Presentation of Adamantinoma With Synchronous 2024 International JouRonald QuezadaNo ratings yet
- Suh 2009Document4 pagesSuh 2009al qurtubi al andalusiNo ratings yet
- Osteosarcoma of The Jaw: Report of 3 Cases (Including The Rare Epithelioid Variant) With Review of LiteratureDocument10 pagesOsteosarcoma of The Jaw: Report of 3 Cases (Including The Rare Epithelioid Variant) With Review of LiteraturesTEVENNo ratings yet
- Clear Cell Odontogenic Carcinoma of The Mandible: A Treatment StrategyDocument5 pagesClear Cell Odontogenic Carcinoma of The Mandible: A Treatment StrategyMaría Fernanda EstévezNo ratings yet
- Unusual Case Report of Concomitant Lunate and Scaph 2024 International JournDocument5 pagesUnusual Case Report of Concomitant Lunate and Scaph 2024 International JournRonald QuezadaNo ratings yet
- Temporal progression of skeletal cystic angiomatosis over 15 yearsDocument6 pagesTemporal progression of skeletal cystic angiomatosis over 15 yearsEma.diazNo ratings yet
- Rare Lumbar Schwannoma CaseDocument5 pagesRare Lumbar Schwannoma CasepetrarizkyNo ratings yet
- Giant Cell Tumor of The Phalanx of Finger: Case Reports: BackgroundDocument10 pagesGiant Cell Tumor of The Phalanx of Finger: Case Reports: BackgroundMoeez AkramNo ratings yet
- GCT ThumbDocument10 pagesGCT ThumbMoeez AkramNo ratings yet
- Anatomo-Radioimaging Correlation in Atypical Ewing SarcomaDocument5 pagesAnatomo-Radioimaging Correlation in Atypical Ewing SarcomaIoana PelinNo ratings yet
- Isolated Lesser Trochanter Fracture Associated With LeukemiaDocument3 pagesIsolated Lesser Trochanter Fracture Associated With LeukemiaIndora DenniNo ratings yet
- Jurnal 2Document5 pagesJurnal 2Centia PicalNo ratings yet
- Fulltext - Smjo v3 1059Document3 pagesFulltext - Smjo v3 1059Rachell AchellNo ratings yet
- Unilateral Mandibular Swelling in A Young Female Patient A Case ReportDocument4 pagesUnilateral Mandibular Swelling in A Young Female Patient A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 2002 Metastatic Renal Cell Carcinoma To The Head and NeckDocument5 pages2002 Metastatic Renal Cell Carcinoma To The Head and NeckAlfonsoSánchezNo ratings yet
- Arthroplasty Today: Case ReportDocument5 pagesArthroplasty Today: Case ReportCristina SavaNo ratings yet
- Giant Cell-Rich Osteosarcoma: A Case ReportDocument7 pagesGiant Cell-Rich Osteosarcoma: A Case ReportRashif AkmalNo ratings yet
- Solitary Plasmacytoma of The Thoracolumbar Spine A Rare Cas - 2022 - InterdisciDocument5 pagesSolitary Plasmacytoma of The Thoracolumbar Spine A Rare Cas - 2022 - Interdiscib00403007No ratings yet
- Tissue of The Causing Referred Pain The Leg: Primary TumoursDocument4 pagesTissue of The Causing Referred Pain The Leg: Primary TumoursantonioopNo ratings yet
- A Rare and Unusual Cause of Discharging Sinus Around The KneeDocument2 pagesA Rare and Unusual Cause of Discharging Sinus Around The KneeRizwan ArshadNo ratings yet
- MRI findings in limb-restricted vasculitisDocument4 pagesMRI findings in limb-restricted vasculitisMithun CbNo ratings yet
- Tuberculosis of The Patella, Report CaseDocument4 pagesTuberculosis of The Patella, Report CaseAnonymous AzXah9n0YNo ratings yet
- A Case of Nodular Fasciitis That Was Difficult To Distinguish From SarcomaDocument5 pagesA Case of Nodular Fasciitis That Was Difficult To Distinguish From SarcomaSotir LakoNo ratings yet
- 71 Full PDFDocument3 pages71 Full PDFshiningdreamNo ratings yet
- Fuchs 2005Document5 pagesFuchs 2005BudhiNo ratings yet
- Orbital Metastasis of A Pediatric Nasopharyngeal Carcinoma A Rare Case ReportDocument4 pagesOrbital Metastasis of A Pediatric Nasopharyngeal Carcinoma A Rare Case ReportInternational Journal of Innovative Science and Research Technology100% (1)
- Research PaperDocument2 pagesResearch PaperMunazzah MehakNo ratings yet
- Hon 2005Document2 pagesHon 2005Andana TrisaviNo ratings yet
- Bilateral Peroneal Tubercle Osteochondroma of The Calcaneus: CaseDocument3 pagesBilateral Peroneal Tubercle Osteochondroma of The Calcaneus: CaseAntony CevallosNo ratings yet
- Management of Non-Metastatic Pelvic Bone Giant Cell Tumour by Resection, Extended Curettage and Reconstruction With Autograft and Allograft - A Case ReportDocument5 pagesManagement of Non-Metastatic Pelvic Bone Giant Cell Tumour by Resection, Extended Curettage and Reconstruction With Autograft and Allograft - A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Journal of Cranio-Maxillo-Facial Surgery: Yehuda Zadik, Alper Aktas, Scott Drucker, Dorrit W. NitzanDocument6 pagesJournal of Cranio-Maxillo-Facial Surgery: Yehuda Zadik, Alper Aktas, Scott Drucker, Dorrit W. Nitzan刘雨樵No ratings yet
- Surgical Treatment of Cyst of The Canal of Nuck and Prevention of Lymphatic Complications: A Single-Center ExperienceDocument6 pagesSurgical Treatment of Cyst of The Canal of Nuck and Prevention of Lymphatic Complications: A Single-Center ExperienceJeje MoNo ratings yet
- PDF KBB 139 PDFDocument4 pagesPDF KBB 139 PDFtriNo ratings yet
- Original Report: MR Imaging Features in Five PatientsDocument4 pagesOriginal Report: MR Imaging Features in Five PatientsEcaterina ChiriacNo ratings yet
- Autopsy 10 4 E2020176Document7 pagesAutopsy 10 4 E2020176PriyakrishnaVasamsettiNo ratings yet
- Spinal Epidural Cavernous Hemangiomas in The 2024 International Journal of SDocument3 pagesSpinal Epidural Cavernous Hemangiomas in The 2024 International Journal of SRonald QuezadaNo ratings yet
- Suprascapular Neuropathy in Volleyball Players: Original StudyDocument4 pagesSuprascapular Neuropathy in Volleyball Players: Original StudyborninbrooklynNo ratings yet
- Keithbidwell 1987Document5 pagesKeithbidwell 1987Ignatius Rheza SetiawanNo ratings yet
- 5 5 5 Pontine Atypical Neurocytoma Case Report 副本Document8 pages5 5 5 Pontine Atypical Neurocytoma Case Report 副本singhNo ratings yet
- TMP EADFDocument5 pagesTMP EADFFrontiersNo ratings yet
- AAOS2002 TumorDocument59 pagesAAOS2002 TumorHizkyas KassayeNo ratings yet
- 1 - Artist Entrance Map - CommencementDocument1 page1 - Artist Entrance Map - CommencementpompompompompomNo ratings yet
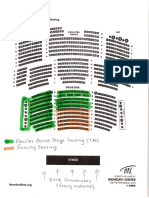
- 6 - FAS Seating MapDocument1 page6 - FAS Seating MappompompompompomNo ratings yet
- Welcome To EMR 440Document1 pageWelcome To EMR 440pompompompompomNo ratings yet
- 01 SISWeb Helpful InformationDocument2 pages01 SISWeb Helpful InformationpompompompompomNo ratings yet
- Safe Glasses Flyer PDFDocument1 pageSafe Glasses Flyer PDFpompompompompomNo ratings yet
- Summer III 3Document1 pageSummer III 3pompompompompomNo ratings yet
- Practice+Midterm+1 - 2Document2 pagesPractice+Midterm+1 - 2pompompompompomNo ratings yet
- Re-Grade Consideration Form For Quiz - : in Your Own WordsDocument1 pageRe-Grade Consideration Form For Quiz - : in Your Own WordspompompompompomNo ratings yet
- AirLift™ Tongue Suspension Technique GuideDocument4 pagesAirLift™ Tongue Suspension Technique GuidedrbudeNo ratings yet
- Spinal Coding HandoutDocument66 pagesSpinal Coding HandoutagnaveenanNo ratings yet
- Dr. Kristia Hermawan, MSC, Sp.A: Pediatric Nephrology Sub-DivisionDocument47 pagesDr. Kristia Hermawan, MSC, Sp.A: Pediatric Nephrology Sub-DivisionWindy MentariNo ratings yet
- Vmax Standard ProtocolDocument5 pagesVmax Standard ProtocolCheeken Charli0% (1)
- W6. Tracheostomy, Introduction To Wound Care & NebulizationDocument4 pagesW6. Tracheostomy, Introduction To Wound Care & NebulizationRHEE ADRIENNE LAI NAVALESNo ratings yet
- Lect 32 Unit IV EndometriosisDocument13 pagesLect 32 Unit IV EndometriosisAsifa BhuttoNo ratings yet
- Cardiovascular Surgery QuizDocument4 pagesCardiovascular Surgery Quizjeevan more100% (2)
- PM TearDocument6 pagesPM TearPiotrek PłotkaNo ratings yet
- DVT Deep Vein ThrombosisDocument19 pagesDVT Deep Vein ThrombosisDoctor MusicNo ratings yet
- Volume 2, Issue 3Document152 pagesVolume 2, Issue 3Asfandyar Sheikh75% (4)
- Cluster 5Document12 pagesCluster 5Eun SaekNo ratings yet
- Bittner 2015 Acute and Perioperative Care of TheDocument34 pagesBittner 2015 Acute and Perioperative Care of TheJuan FelipeNo ratings yet
- Topographic and Neural Anatomy of The Depressor Anguli Oris Muscle and Implications For Treatment of Synkinectic Facial ParalysisDocument11 pagesTopographic and Neural Anatomy of The Depressor Anguli Oris Muscle and Implications For Treatment of Synkinectic Facial ParalysisJohn NinNo ratings yet
- VAD Patient Education ManualDocument12 pagesVAD Patient Education ManualIakovos DanielosNo ratings yet
- IJISRT23JUN363Document7 pagesIJISRT23JUN363International Journal of Innovative Science and Research TechnologyNo ratings yet
- NG Tube FeedingDocument3 pagesNG Tube FeedingMaheswari BossNo ratings yet
- Toprank Review Pediatric Nursing Notes CompressDocument13 pagesToprank Review Pediatric Nursing Notes CompressMaria Ana AguilarNo ratings yet
- Right and Extended Right ColectomyDocument19 pagesRight and Extended Right Colectomybo gum parkNo ratings yet
- D-Dimer 12Document7 pagesD-Dimer 12محمد عماد علي احمدNo ratings yet
- Phacoemulsification & Extra Capsular Cataract ExtractionDocument7 pagesPhacoemulsification & Extra Capsular Cataract ExtractionJo-anne CorderoNo ratings yet
- Hospital Practice & Patient CareDocument14 pagesHospital Practice & Patient CareAkinsola Ayomidotun100% (1)
- Preparing A Patient For SurgeryDocument2 pagesPreparing A Patient For SurgeryVinnes Ann InfanteNo ratings yet
- Acute Stroke Case: Rapid Identification and Initial ManagementDocument19 pagesAcute Stroke Case: Rapid Identification and Initial ManagementAsep BageurNo ratings yet
- Olav Istre (Eds.) - Minimally Invasive Gynecological Surgery-Springer-Verlag Berlin Heidelberg (2015)Document201 pagesOlav Istre (Eds.) - Minimally Invasive Gynecological Surgery-Springer-Verlag Berlin Heidelberg (2015)ravikanth100% (1)
- Drain CareDocument6 pagesDrain Carecharleston_mendozaNo ratings yet
- Complex Protrombina Huvh 01 10Document11 pagesComplex Protrombina Huvh 01 10Santiago Rodriguez MoralesNo ratings yet
- Surgical Atlas Transureteroureterostomy: John M. BarryDocument7 pagesSurgical Atlas Transureteroureterostomy: John M. BarrycristiangelsNo ratings yet
- Iassacon 2018 SP 23022018 Finalwithouthall 2 Ic 6Document4 pagesIassacon 2018 SP 23022018 Finalwithouthall 2 Ic 6ishu sNo ratings yet
- Robotic Bronchoscopy For Pulmonary Lesions A RevieDocument8 pagesRobotic Bronchoscopy For Pulmonary Lesions A RevieAlaaNo ratings yet
- ACL Reconstruction With BTB TightRopeDocument6 pagesACL Reconstruction With BTB TightRopeGustavo Enrique Matson CarballoNo ratings yet