You might also like
- The Development and Application of A New Tool The Content and Timing ANCDocument10 pagesThe Development and Application of A New Tool The Content and Timing ANCFarhatiNo ratings yet
- Determining The Determinants of Health Behavior ChangeDocument13 pagesDetermining The Determinants of Health Behavior ChangeFarhatiNo ratings yet
- Designing Digital InterventionsDocument93 pagesDesigning Digital InterventionsFarhati100% (1)
- Internet Health Promotion and Behavior Change Theory An IntegratedDocument6 pagesInternet Health Promotion and Behavior Change Theory An IntegratedFarhatiNo ratings yet
- Assessing The Impact of MHealth Interventions in Low and Middle Income CountryDocument12 pagesAssessing The Impact of MHealth Interventions in Low and Middle Income CountryFarhatiNo ratings yet
- Daftar Tilik APN Sesuai MU 2016Document7 pagesDaftar Tilik APN Sesuai MU 2016FarhatiNo ratings yet
- Quality Issu in Midwifery ICM PDFDocument9 pagesQuality Issu in Midwifery ICM PDFFarhatiNo ratings yet
- Current Mhealth Technologies For Physical Activity Assessment PDFDocument13 pagesCurrent Mhealth Technologies For Physical Activity Assessment PDFFarhatiNo ratings yet
- Improving Access To Quality Marternal and Child Health Service PDFDocument11 pagesImproving Access To Quality Marternal and Child Health Service PDFFarhatiNo ratings yet
- Jurnal Pelayanan ANC Di KENYADocument10 pagesJurnal Pelayanan ANC Di KENYAFarhatiNo ratings yet
- Internet Use by Pregnant Women Seeking PDFDocument10 pagesInternet Use by Pregnant Women Seeking PDFFarhatiNo ratings yet
- Information, Education and Communication: OccasionalDocument42 pagesInformation, Education and Communication: OccasionalFarhatiNo ratings yet
- Associations Between Characteristics of The HomeDocument10 pagesAssociations Between Characteristics of The HomeFarhatiNo ratings yet
- A Systematic Review of Types of Healthy Eating Interventions in PreschoolsDocument20 pagesA Systematic Review of Types of Healthy Eating Interventions in PreschoolsFarhatiNo ratings yet
- Quality Issu in Midwifery ICMDocument9 pagesQuality Issu in Midwifery ICMFarhati100% (1)
- Compliance With Focused Antenatal Care Services Do HealthDocument8 pagesCompliance With Focused Antenatal Care Services Do HealthFarhatiNo ratings yet
- Leg Cramps The Underlying PDFDocument3 pagesLeg Cramps The Underlying PDFFarhatiNo ratings yet
- Nutritional Intervention For Muscle CrampsDocument5 pagesNutritional Intervention For Muscle CrampsFarhatiNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Lab # 5 Use Case and Activity Diagram: ObjectivesDocument7 pagesLab # 5 Use Case and Activity Diagram: ObjectivesmexiweNo ratings yet
- Drugs of Autonomic Nervous SystemDocument34 pagesDrugs of Autonomic Nervous SystemWyz Class100% (1)
- Vi. Nursing Care PlanDocument11 pagesVi. Nursing Care PlanSamantha BolanteNo ratings yet
- Complete Guide To Communication Problems After StrokeDocument22 pagesComplete Guide To Communication Problems After Strokeapi-215453798100% (1)
- Sagar SinghDocument4 pagesSagar SinghzombieNo ratings yet
- 中考英语100篇满分作文精讲(附万能写作句子)Document109 pages中考英语100篇满分作文精讲(附万能写作句子)qrh1950623825No ratings yet
- Grade 9 Solid Waste Management Teachers - GuideDocument32 pagesGrade 9 Solid Waste Management Teachers - GuideNicole Angela NavarroNo ratings yet
- Department of Education: Granja Kalinawan National High SchoolDocument26 pagesDepartment of Education: Granja Kalinawan National High SchoolRoselyn Mae DulaNo ratings yet
- Waiver FormDocument2 pagesWaiver Formapi-249429435No ratings yet
- Cinnamon: Material Safety Data SheetDocument4 pagesCinnamon: Material Safety Data SheetJohn AnthraperNo ratings yet
- The Emergence of India's Pharmaceutical IndustryDocument41 pagesThe Emergence of India's Pharmaceutical Industryvivekgupta2jNo ratings yet
- PuppetryDocument183 pagesPuppetryÉva Hegedüsné50% (2)
- Abnormal Illness BehaviorDocument7 pagesAbnormal Illness Behavioransha2011p0% (1)
- Research Proposal-1Document28 pagesResearch Proposal-1sowsthikaNo ratings yet
- Health and Wellbeing: AT WORK 2021Document37 pagesHealth and Wellbeing: AT WORK 2021Constantin CiacaruNo ratings yet
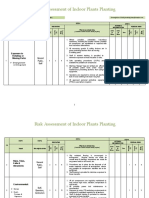
- Risk Assessment of Indoor Plants PlantingDocument5 pagesRisk Assessment of Indoor Plants Plantingطارق رضوانNo ratings yet
- Curriculum Vitae - Aditya Pratama PutraDocument3 pagesCurriculum Vitae - Aditya Pratama PutraIan SeptiantoNo ratings yet
- Xcelera Brochure Updated (English)Document24 pagesXcelera Brochure Updated (English)Pablo Rosas100% (1)
- Fans Instructions CE (A015)Document72 pagesFans Instructions CE (A015)vasaNo ratings yet
- Zika Virus and PregnancyDocument5 pagesZika Virus and PregnancyHerryNo ratings yet
- Prevalence of High Risk Pregnancy in Rural DharwadDocument4 pagesPrevalence of High Risk Pregnancy in Rural DharwadIOSRjournalNo ratings yet
- Complete Holistic Guide To Working Out in The GymDocument218 pagesComplete Holistic Guide To Working Out in The Gympsichi21No ratings yet
- UJA-Federation of New York Donor Recognition List 2022Document17 pagesUJA-Federation of New York Donor Recognition List 2022ericlkaplanNo ratings yet
- Subject: PsychopharmacologyDocument11 pagesSubject: PsychopharmacologyAli IjazNo ratings yet
- Basics of Therapeutic DietsDocument12 pagesBasics of Therapeutic DietstiruchanurNo ratings yet
- CrimPro Cases (Rule 116)Document45 pagesCrimPro Cases (Rule 116)elvinperiaNo ratings yet
- Curriculum Vitae: Personal InformationDocument4 pagesCurriculum Vitae: Personal InformationajmanNo ratings yet
- Zinc in Wound Healing Theoretical, ExperimentalDocument15 pagesZinc in Wound Healing Theoretical, ExperimentalRifky Budi TriyatnoNo ratings yet
- Rajasthan Hospitals LISTDocument19 pagesRajasthan Hospitals LISTOrigin Over100% (1)
- Brochure Philippine Laws On Environmental PollutionDocument8 pagesBrochure Philippine Laws On Environmental PollutionElvin JuniorNo ratings yet