You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- MITcasebook ConsultingDocument173 pagesMITcasebook Consultingjtien512100% (10)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Sample Custom Iphone App Development Agreement Custom Software Development Agreement PDFDocument7 pagesSample Custom Iphone App Development Agreement Custom Software Development Agreement PDFLevale XrNo ratings yet
- Speed in The Third ReichDocument14 pagesSpeed in The Third ReichJohn Hurley100% (1)
- HRM Case StudyDocument2 pagesHRM Case StudyVikas Sharma100% (3)
- TBRw6 ResourcesPublication FINALDocument1 pageTBRw6 ResourcesPublication FINALcallmedump1No ratings yet
- TBRw6 EligibleCountries FINALDocument1 pageTBRw6 EligibleCountries FINALcallmedump1No ratings yet
- CBNAAT Implementati - Challenges & RecommendationsDocument6 pagesCBNAAT Implementati - Challenges & Recommendationscallmedump1No ratings yet
- TBRw6 CatalyticFunding FINALDocument2 pagesTBRw6 CatalyticFunding FINALcallmedump1No ratings yet
- 2011 D05 00 ProvDocument6 pages2011 D05 00 Provcallmedump1No ratings yet
- TBRw6 ProcessTimeline FINALDocument1 pageTBRw6 ProcessTimeline FINALcallmedump1No ratings yet
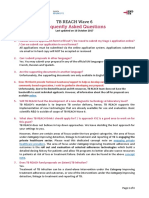
- Tbrw6 Faq FinalDocument4 pagesTbrw6 Faq Finalcallmedump1No ratings yet
- TB India 2017Document173 pagesTB India 2017dratultiwariNo ratings yet
- Sensitivity & SpecificityDocument1 pageSensitivity & Specificitycallmedump1No ratings yet
- A-1 No of Villages Towns Households Population and AreaDocument890 pagesA-1 No of Villages Towns Households Population and Areacallmedump1No ratings yet
- Key Population BriefDocument27 pagesKey Population Briefcallmedump1No ratings yet
- Sops - Usaid Layout Program Evaulation, Performance Measurement Approach Duplication Between TGF and Usaid CitiesDocument1 pageSops - Usaid Layout Program Evaulation, Performance Measurement Approach Duplication Between TGF and Usaid Citiescallmedump1No ratings yet
- ID India Ppia Fs r1Document2 pagesID India Ppia Fs r1callmedump1No ratings yet
- PIP - Norms and Basis of CostingDocument12 pagesPIP - Norms and Basis of Costingcallmedump1No ratings yet
- 909090Document64 pages909090callmedump1No ratings yet
- Equipment Management OrissaDocument125 pagesEquipment Management Orissacallmedump1No ratings yet
- Estimation of Child Vaccination CoverageDocument13 pagesEstimation of Child Vaccination Coveragecallmedump1No ratings yet
- Disadvantaged Groups DefinitionDocument6 pagesDisadvantaged Groups Definitioncallmedump1No ratings yet
- Molecular Line Probe Assays For Rapid Screening of Patients at Risk of Multidrug-Resistant TuberculosisDocument9 pagesMolecular Line Probe Assays For Rapid Screening of Patients at Risk of Multidrug-Resistant Tuberculosiscallmedump1No ratings yet
- DSF No27IEGDocument34 pagesDSF No27IEGcallmedump1No ratings yet
- CAD Software For X-Ray ScreeningDocument2 pagesCAD Software For X-Ray Screeningcallmedump1No ratings yet
- Cold Chain ManagementDocument37 pagesCold Chain Managementcallmedump1No ratings yet
- Consuming Bhuvan Services QgisDocument5 pagesConsuming Bhuvan Services Qgiscallmedump1No ratings yet
- Bhuvan User HandbookDocument92 pagesBhuvan User Handbookcallmedump1No ratings yet
- ChaptersDocument34 pagesChapterscallmedump1No ratings yet
- PPP Task Force Report-DraftDocument41 pagesPPP Task Force Report-DraftSudhir SinghNo ratings yet
- Common Pros2016Document192 pagesCommon Pros2016erickaa3010No ratings yet
- Foss For BhuvanDocument20 pagesFoss For Bhuvancallmedump1No ratings yet
- Alcon 2010 20-FDocument257 pagesAlcon 2010 20-Fds__scribdNo ratings yet
- Drugs and Devices: Comparison of European and U.S. Approval ProcessesDocument14 pagesDrugs and Devices: Comparison of European and U.S. Approval ProcessesJagdish ChanderNo ratings yet
- JSB IntelligenceDocument82 pagesJSB Intelligenceanuraggau0% (1)
- Apex Pharmaceutical Marketing AssaignmentDocument19 pagesApex Pharmaceutical Marketing Assaignmenti_simanto_iNo ratings yet
- NS Camp 2012 - Health History Form For HTsDocument1 pageNS Camp 2012 - Health History Form For HTsThanhThao NguyenNo ratings yet
- Antifoams ChartDocument1 pageAntifoams ChartTariq Khan OtmanzaiNo ratings yet
- Management Report On Square Pharmaceuticals LTDDocument17 pagesManagement Report On Square Pharmaceuticals LTDNiladri HasanNo ratings yet
- Letter of Compliance Inspection FormDocument5 pagesLetter of Compliance Inspection Formabc2newsNo ratings yet
- Marketing Plan B6 BioconDocument9 pagesMarketing Plan B6 BioconRitvik DineshNo ratings yet
- Vocabular CuvinteDocument10 pagesVocabular CuvinteAlina-elena Micevski-ignatNo ratings yet
- Orange BookDocument43 pagesOrange BookbiosiriNo ratings yet
- Cymbalta Final - 70682643 PDFDocument11 pagesCymbalta Final - 70682643 PDFemanuelariobimoNo ratings yet
- The Pharmaceutical Industry: Career Opportunities For PharmacistsDocument8 pagesThe Pharmaceutical Industry: Career Opportunities For PharmacistsHanan AhmedNo ratings yet
- HmisDocument14 pagesHmis166873100% (1)
- Fall Tips Toolkit Mfs Training ModuleDocument20 pagesFall Tips Toolkit Mfs Training ModulenindhiapvNo ratings yet
- Healthcare in BDDocument20 pagesHealthcare in BDAl AminNo ratings yet
- Managing The Health Care Supply ChainDocument18 pagesManaging The Health Care Supply ChainHanan AhmedNo ratings yet
- Algeria Pharma MarketDocument55 pagesAlgeria Pharma Marketvdved67% (3)
- Nestle Pure Life Bottled WaterDocument20 pagesNestle Pure Life Bottled WaterFreedomFighter32No ratings yet
- Institute For Safe Medication PracticesDocument6 pagesInstitute For Safe Medication Practicesadza30No ratings yet
- Agp Ipo2016Document12 pagesAgp Ipo2016rafeel0% (1)
- Toxicology Clinical PharmacyDocument18 pagesToxicology Clinical Pharmacyxtremist2001100% (4)
- MC Tradit Medicinal Plants TZ en LP 138650Document620 pagesMC Tradit Medicinal Plants TZ en LP 138650kumargautambkscNo ratings yet
- BibliographyDocument2 pagesBibliographyMahesh T MadhavanNo ratings yet
- Session III Ichq6b SpecificationsDocument84 pagesSession III Ichq6b Specificationsamandbhaskar100% (1)
- Feasibility of Active Pharmaceutical Ingredient (API) Industry by Imrul Sadat, HTTPDocument4 pagesFeasibility of Active Pharmaceutical Ingredient (API) Industry by Imrul Sadat, HTTPAnonymous zItwm5No ratings yet
- S20282en PDFDocument192 pagesS20282en PDFAnonymous CR8v7xb0No ratings yet