You might also like
- ObobDocument1 pageObobNikkie SalazarNo ratings yet
- Prevalence and Risk Factors of Diabetic Foot Ulcer at A Tertiary Care Hospital Among Diabetic PatientsDocument6 pagesPrevalence and Risk Factors of Diabetic Foot Ulcer at A Tertiary Care Hospital Among Diabetic PatientsNikkie SalazarNo ratings yet
- AgikDocument4 pagesAgikNikkie SalazarNo ratings yet
- Professional Adjustment: Mila Delia M. Llanes, PHD, RN Ust College of NursingDocument45 pagesProfessional Adjustment: Mila Delia M. Llanes, PHD, RN Ust College of NursingNikkie SalazarNo ratings yet
- Gynecology Case: Rily Sedentary ActivitiesDocument1 pageGynecology Case: Rily Sedentary ActivitiesNikkie SalazarNo ratings yet
- Nursing Laws & RegulationsDocument46 pagesNursing Laws & RegulationsNikkie Salazar100% (1)
- PedsDocument16 pagesPedsNikkie SalazarNo ratings yet
- Intra PartumDocument2 pagesIntra PartumNikkie SalazarNo ratings yet
- PostpartumDocument1 pagePostpartumNikkie SalazarNo ratings yet
- Sigmund Freud TheoryDocument4 pagesSigmund Freud TheoryNikkie SalazarNo ratings yet
- Nurse Practice Act1Document20 pagesNurse Practice Act1Nikkie SalazarNo ratings yet
- Nurse Practice Act1Document1 pageNurse Practice Act1Nikkie SalazarNo ratings yet
- Professional AdjustmentDocument12 pagesProfessional AdjustmentNikkie Salazar100% (1)
- Laws Affecting The Practice of Nursing in The PhilippinesDocument3 pagesLaws Affecting The Practice of Nursing in The PhilippinesMeynard AndresNo ratings yet
- Legal Liabilities in Nursing PracticeDocument66 pagesLegal Liabilities in Nursing PracticeNikkie SalazarNo ratings yet
- Nurse Practice Act1Document20 pagesNurse Practice Act1Nikkie SalazarNo ratings yet
- Nurse Performs Neurologic ChecksDocument5 pagesNurse Performs Neurologic ChecksNikkie SalazarNo ratings yet
- Code of Good Governance for Professions in the PhilippinesDocument10 pagesCode of Good Governance for Professions in the PhilippinesNikkie SalazarNo ratings yet
- Coin Sorting Machine: Cainta Catholic College Grade School Department Cainta, Rizal A.Y 2018-2019Document3 pagesCoin Sorting Machine: Cainta Catholic College Grade School Department Cainta, Rizal A.Y 2018-2019Nikkie SalazarNo ratings yet
- XXXasasDocument2 pagesXXXasasNikkie SalazarNo ratings yet
- Step Project Proposal Edited VersionDocument14 pagesStep Project Proposal Edited VersionNikkie SalazarNo ratings yet
- The Origin of The Holy RosaryDocument5 pagesThe Origin of The Holy RosaryNikkie SalazarNo ratings yet
- Name of Corporation: Personal Information SheetDocument4 pagesName of Corporation: Personal Information SheetNikkie SalazarNo ratings yet
- Coinsorting MachineDocument3 pagesCoinsorting MachineNikkie SalazarNo ratings yet
- Senior Project Proposal Form SAMPLEDocument8 pagesSenior Project Proposal Form SAMPLENikkie SalazarNo ratings yet
- 1 s2.0 S1878875017319708 MainDocument4 pages1 s2.0 S1878875017319708 MainNikkie SalazarNo ratings yet
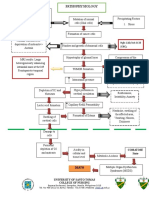
- Ependymomas Are Brain Tumors That Arise From Ependymal CellsDocument1 pageEpendymomas Are Brain Tumors That Arise From Ependymal CellsNikkie SalazarNo ratings yet
- Project Proposal 1Document2 pagesProject Proposal 1Anonymous sZLcBAgNo ratings yet
- CV Template OutlineDocument6 pagesCV Template OutlineFotis TsamisNo ratings yet
- 1 s2.0 S1878875017319708 MainDocument4 pages1 s2.0 S1878875017319708 MainNikkie SalazarNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 50 Cool Stories 3000 Hot Words (Master Vocabulary in 50 Days) For GRE Mba Sat Banking SSC DefDocument263 pages50 Cool Stories 3000 Hot Words (Master Vocabulary in 50 Days) For GRE Mba Sat Banking SSC DefaravindNo ratings yet
- Psychology - A Separate PeaceDocument2 pagesPsychology - A Separate PeacevasudhaaaaaNo ratings yet
- Lecture Notes 1-8Document39 pagesLecture Notes 1-8Mehdi MohmoodNo ratings yet
- Culture of BMWDocument6 pagesCulture of BMWhk246100% (1)
- Louis Theroux PowerpointDocument6 pagesLouis Theroux Powerpointapi-330762792No ratings yet
- Tle-Bpp 8-Q1-M18Document14 pagesTle-Bpp 8-Q1-M18Michelle LlanesNo ratings yet
- Lung BiopsyDocument8 pagesLung BiopsySiya PatilNo ratings yet
- GII-07 Training MaterialDocument191 pagesGII-07 Training MaterialIris Amati MartinsNo ratings yet
- Ch.24.2 Animal Evolution and DiversityDocument34 pagesCh.24.2 Animal Evolution and DiversityweldeenytNo ratings yet
- Autism AspergerDocument24 pagesAutism AspergerusavelNo ratings yet
- Longman - New Total English Elementary Video BankDocument26 pagesLongman - New Total English Elementary Video Bankyuli100% (1)
- Havighurst ThePirenneThesis (BW)Document133 pagesHavighurst ThePirenneThesis (BW)tmarr014100% (1)
- Chapter 9 MafinDocument36 pagesChapter 9 MafinReymilyn SanchezNo ratings yet
- VDA ChinaDocument72 pagesVDA Chinatuananh1010No ratings yet
- Ash ContentDocument2 pagesAsh Contentvikasbnsl1No ratings yet
- Christian Storytelling EvaluationDocument3 pagesChristian Storytelling Evaluationerika paduaNo ratings yet
- The Role of Christian Education in Socia Group 6Document6 pagesThe Role of Christian Education in Socia Group 6Ṭhanuama BiateNo ratings yet
- Literature - Part I: Group InterventionsDocument14 pagesLiterature - Part I: Group InterventionsDanielNo ratings yet
- Answer Here:: FAMILY NAME - FIRST NAME - CLASSCODEDocument4 pagesAnswer Here:: FAMILY NAME - FIRST NAME - CLASSCODEUchayyaNo ratings yet
- Chap 4 eDocument22 pagesChap 4 eHira AmeenNo ratings yet
- Universitas Alumni Psikotest LolosDocument11 pagesUniversitas Alumni Psikotest LolosPsikotes BVKNo ratings yet
- Formula Sheet For Astronomy 1 - Paper 1 and Stars & PlanetsDocument2 pagesFormula Sheet For Astronomy 1 - Paper 1 and Stars & PlanetsprashinNo ratings yet
- The Forty Nine StepsDocument312 pagesThe Forty Nine Stepsoldnic67% (3)
- The Army Crew Team Case AnalysisDocument3 pagesThe Army Crew Team Case Analysisarshdeep199075% (4)
- The BrigadeDocument517 pagesThe Brigadele_chiffre4860100% (3)
- Parashara'S Light 7.0.1 (C) Geovision Software, Inc., Licensed ToDocument5 pagesParashara'S Light 7.0.1 (C) Geovision Software, Inc., Licensed TobrajwasiNo ratings yet
- Sengoku WakthroughDocument139 pagesSengoku WakthroughferdinanadNo ratings yet
- 3B Adverbial PhrasesDocument1 page3B Adverbial PhrasesSarah INo ratings yet
- ViscosityDocument7 pagesViscositykiran2381No ratings yet
- People vs. Abad SantosDocument2 pagesPeople vs. Abad SantosTrixie PeraltaNo ratings yet