You might also like
- The Art of Stage Dancing The Story of a Beautiful and Profitable ProfessionFrom EverandThe Art of Stage Dancing The Story of a Beautiful and Profitable ProfessionNo ratings yet
- Contact Sheet For TheatreDocument7 pagesContact Sheet For TheatreLancelot du LacNo ratings yet
- Sp16 Musical Audition FormDocument2 pagesSp16 Musical Audition FormKim PerniaNo ratings yet
- Playbill Grease Final Compressed PicturesDocument28 pagesPlaybill Grease Final Compressed Picturesapi-365574700No ratings yet
- Pre Show ChecklistDocument1 pagePre Show Checklistapi-279708967No ratings yet
- Us Musical Audition FormDocument3 pagesUs Musical Audition Formapi-242444649No ratings yet
- Rehearsal Report 1Document1 pageRehearsal Report 1api-273020603No ratings yet
- Hamilton 3 PDFDocument4 pagesHamilton 3 PDFcreampinkNo ratings yet
- MUGN 212 ScheduleDocument5 pagesMUGN 212 SchedulegothicoboistNo ratings yet
- 1950s When Broadway RuledDocument17 pages1950s When Broadway RuledAdrian BarilàNo ratings yet
- Cglen@Indiana - Edu Lya@Iu - Edu: Wwnorton, 2011. 978-0-393-92906-5Document12 pagesCglen@Indiana - Edu Lya@Iu - Edu: Wwnorton, 2011. 978-0-393-92906-5singermzNo ratings yet
- History of Classical Music PDFDocument55 pagesHistory of Classical Music PDFJohannJoeAguirreNo ratings yet
- Tap Dancer ProjectDocument4 pagesTap Dancer ProjectCaleb GrochalskiNo ratings yet
- Musician Resume SampleDocument1 pageMusician Resume Samplevijaymusic88No ratings yet
- Jackie and Me Study GuideDocument20 pagesJackie and Me Study GuideChildren's Theatre CompanyNo ratings yet
- Parts of A ProductionDocument19 pagesParts of A ProductionKeira GatenbyNo ratings yet
- Theatre Audition PacketDocument8 pagesTheatre Audition PacketashleybostromNo ratings yet
- Little Shop Program2 2Document28 pagesLittle Shop Program2 2api-245424423No ratings yet
- Broadway GlossaryDocument6 pagesBroadway GlossaryPhoebe JacksonNo ratings yet
- The Conductorless OrchestraDocument10 pagesThe Conductorless OrchestraHarvey SeifterNo ratings yet
- Popovers in Dorico: Bars and Barlines (Shift+B)Document13 pagesPopovers in Dorico: Bars and Barlines (Shift+B)Palanisamy Balasubramani100% (1)
- Acting Syllabus Specifications From 2023 - ONLINEDocument106 pagesActing Syllabus Specifications From 2023 - ONLINEKhyati RajaNo ratings yet
- Composer Research ProjectDocument4 pagesComposer Research Projectapi-265352428No ratings yet
- Technical Theatre SyllabusDocument2 pagesTechnical Theatre Syllabusapi-369620975100% (1)
- Title of Show Study GuideDocument11 pagesTitle of Show Study GuideJuran JonesNo ratings yet
- Sponsorship Letter For Golden Arches Development Corp.Document6 pagesSponsorship Letter For Golden Arches Development Corp.Riemann SolivenNo ratings yet
- Audition Sheet (Resume) : List Theatre Experience (Classes Plays)Document1 pageAudition Sheet (Resume) : List Theatre Experience (Classes Plays)BrandonKirklenNo ratings yet
- Games in A Theatre ClassroomDocument17 pagesGames in A Theatre Classroomajayshandilya4309No ratings yet
- THEA 80N Walt Disney SyllabusDocument2 pagesTHEA 80N Walt Disney SyllabusLilo YoungNo ratings yet
- Secondary Unit PlanDocument4 pagesSecondary Unit Planapi-643485262No ratings yet
- Grease Show ResearchDocument4 pagesGrease Show ResearchAndrew MartiniNo ratings yet
- Young Frankenstein Seattle InfoDocument3 pagesYoung Frankenstein Seattle InfoAndrey KiselevNo ratings yet
- Music Theory HandoutDocument3 pagesMusic Theory HandoutpugandjNo ratings yet
- History of Musical Theater Lesson PlanDocument2 pagesHistory of Musical Theater Lesson Planapi-215912697No ratings yet
- Music Analysis WorksheetDocument2 pagesMusic Analysis WorksheetPhilip ArgauerNo ratings yet
- Drama 252 Spring 2017 SyllabusDocument6 pagesDrama 252 Spring 2017 SyllabusElliott ChinnNo ratings yet
- What To Know Before You Go - EaglesGNRDocument4 pagesWhat To Know Before You Go - EaglesGNRHNNNo ratings yet
- Rehearsal Technique/Rehearsal Etique!e: Be Present and On TimeDocument2 pagesRehearsal Technique/Rehearsal Etique!e: Be Present and On TimeBryan SibbittsNo ratings yet
- Tech Fundamentals - Syllabus - FallDocument3 pagesTech Fundamentals - Syllabus - Fallapi-261377026100% (1)
- Pharmacon Alien ScoreDocument45 pagesPharmacon Alien ScoreDeborah LewisNo ratings yet
- TH e Golde N Ag E O F Musicals: 1 2 0 To 196 0Document2 pagesTH e Golde N Ag E O F Musicals: 1 2 0 To 196 0Nathan PoetschkaNo ratings yet
- "Violet" The Musical Keys 3 Patch ListDocument5 pages"Violet" The Musical Keys 3 Patch ListCasey on the KeysNo ratings yet
- High School Musical 2014 Schedule 2Document3 pagesHigh School Musical 2014 Schedule 2api-262819683No ratings yet
- Porgy and Bess: Opera in Two ActsDocument24 pagesPorgy and Bess: Opera in Two ActsInverted Human100% (1)
- Broadway 1950's - 1990's: Area of Study 2Document7 pagesBroadway 1950's - 1990's: Area of Study 2tph103No ratings yet
- USO Show ScriptDocument3 pagesUSO Show ScriptMelina WorthingtonNo ratings yet
- Theatre Design BookletDocument43 pagesTheatre Design BookletEvie TantramNo ratings yet
- Merrily We Roll AlongDocument2 pagesMerrily We Roll AlongMeshack O SindaniNo ratings yet
- She Loves Me BreakdownDocument2 pagesShe Loves Me BreakdownMichelle ZinkNo ratings yet
- Actors ' Equity Actors ' Etiquette: Ctors Quity SsociationDocument2 pagesActors ' Equity Actors ' Etiquette: Ctors Quity SsociationEmelia CappelliNo ratings yet
- Shout Musical Theater BlitzsteinDocument17 pagesShout Musical Theater BlitzsteinRichardRobbinsNo ratings yet
- Jeb The MusicalDocument149 pagesJeb The Musicalnrhuff1995No ratings yet
- Chorus Line (Pioneer) Study GuideDocument4 pagesChorus Line (Pioneer) Study GuideHilly McChefNo ratings yet
- Props List TemplateDocument2 pagesProps List TemplateSamuel BamfoNo ratings yet
- Grease Rehearsal Schedule 1Document9 pagesGrease Rehearsal Schedule 1Nicholas RollandNo ratings yet
- Cte Portfolio Production Syllabus - StudentDocument5 pagesCte Portfolio Production Syllabus - Studentapi-261377026No ratings yet
- Wiz Choreography NotesDocument3 pagesWiz Choreography Noteskec678No ratings yet
- Theatre One-SheetDocument2 pagesTheatre One-Sheetapi-313390750No ratings yet
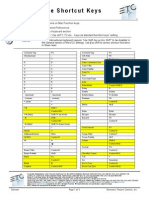
- ETC Console Shortcut Keys: Element v2.3.0Document3 pagesETC Console Shortcut Keys: Element v2.3.0Hello aksNo ratings yet
- Timor PC Guidebook2Document402 pagesTimor PC Guidebook2Ralph Perez100% (1)
- First You DreamDocument11 pagesFirst You DreamRalph PerezNo ratings yet
- Flueggea Flexuosa (Poumuli) : Species Profiles For Pacific Island AgroforestryDocument13 pagesFlueggea Flexuosa (Poumuli) : Species Profiles For Pacific Island AgroforestryRalph Perez100% (1)
- Everlasting Light Design Direction: Production ConceptDocument2 pagesEverlasting Light Design Direction: Production ConceptRalph PerezNo ratings yet
- Forces of Nature ProgramDocument11 pagesForces of Nature ProgramRalph PerezNo ratings yet
- Conducting CourseDocument106 pagesConducting CourseDennis Vigil Caballero100% (3)
- Ernest Douglas AHS Memory BookDocument34 pagesErnest Douglas AHS Memory BookDru WrightNo ratings yet
- Band Grading RubricDocument1 pageBand Grading Rubricapi-263741380No ratings yet
- Lip Sync AssignmentDocument3 pagesLip Sync Assignmentapi-400083875No ratings yet
- Resume GremsDocument2 pagesResume Gremsapi-353964625No ratings yet
- Music Assistants Sop 1-6-2022Document13 pagesMusic Assistants Sop 1-6-2022John NorineNo ratings yet
- Basic Theatre Terminology: Fundamentals of Theatre IDocument46 pagesBasic Theatre Terminology: Fundamentals of Theatre IRhen BorjaNo ratings yet
- The Little Sweep - VocalScoreDocument100 pagesThe Little Sweep - VocalScoreJosy100% (1)
- ĐỀ THI THỬ SỐ 43- KHÓA 8+ NGÀY 06062022-BIÊN SOẠN CÔ PHẠM LIỄUDocument8 pagesĐỀ THI THỬ SỐ 43- KHÓA 8+ NGÀY 06062022-BIÊN SOẠN CÔ PHẠM LIỄUKhánh ThiNo ratings yet
- Role of Music in WorshipDocument12 pagesRole of Music in WorshipMaurice Dan GeroyNo ratings yet
- The Rehearsal Techniques of Robert Shaw: Essential Building BlocksDocument5 pagesThe Rehearsal Techniques of Robert Shaw: Essential Building Blocksarnoldlee1No ratings yet
- Roles of in A Stage ProductionDocument1 pageRoles of in A Stage ProductionAshley Nicole CustodioNo ratings yet
- Durrant 2005 - Shaping Identity Through Choral Activities Singers and Conductors PerceptionsDocument11 pagesDurrant 2005 - Shaping Identity Through Choral Activities Singers and Conductors PerceptionsLucas TossNo ratings yet
- Rehearsal Observation PDFDocument2 pagesRehearsal Observation PDFMason FrasherNo ratings yet
- Speech and Theater Arts QuestionsDocument4 pagesSpeech and Theater Arts QuestionsNavarro Jeremiah S.No ratings yet
- Choral Rehearsal TechniquesDocument2 pagesChoral Rehearsal Techniquesrdwilson412100% (2)
- Oxford Handbooks Online: The Choral Experience: Turned Inside OutDocument20 pagesOxford Handbooks Online: The Choral Experience: Turned Inside OutPatricio Emiliano Vega GómezNo ratings yet
- Webb 2007 Promoting Vocal Health in The Choral RehearsalDocument6 pagesWebb 2007 Promoting Vocal Health in The Choral RehearsalDiana SilvaNo ratings yet
- Advanced Directing TipsDocument8 pagesAdvanced Directing TipsBogdan Theodor OlteanuNo ratings yet
- Site-Specific Mini-UnitDocument7 pagesSite-Specific Mini-Unitapi-334499622No ratings yet
- Unit 6b Music LogbookDocument42 pagesUnit 6b Music Logbookapi-200177496No ratings yet
- Drama Study GuideDocument17 pagesDrama Study GuideMelody WolfeNo ratings yet
- 2nd Term Cca jss2Document25 pages2nd Term Cca jss2yahqoob abdulrasheed100% (1)
- Dramatic Arts Trial Exam 2023 - GR12Document8 pagesDramatic Arts Trial Exam 2023 - GR12semoneNo ratings yet
- 2022 2023 Middle School Musical Theatre SyllabusDocument5 pages2022 2023 Middle School Musical Theatre Syllabusamya733468No ratings yet
- Ethic in Ensemble Performance Assignment (Zulhariz)Document4 pagesEthic in Ensemble Performance Assignment (Zulhariz)Rodney Aldo RaymondNo ratings yet
- Fili ContentDocument46 pagesFili ContentJoe Louie Agoncillo LavaroNo ratings yet
- Collaborative Piano-Oh The Places You WilDocument7 pagesCollaborative Piano-Oh The Places You WilLuiza Mathias100% (1)
- CV Morgan White - ResumeDocument3 pagesCV Morgan White - Resumeapi-610297695No ratings yet
- Student Clubs Detailed Packet 11-12.Document10 pagesStudent Clubs Detailed Packet 11-12.RMHSMarconiNo ratings yet