You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Faktor Faktor Yang Berhubungan Dengan Perilaku Penggunaan Alat Kontrasepsi Non Mket Pada Wus Peserta KB Aktif Di Kecamatan Oebobo Kota KupangDocument8 pagesFaktor Faktor Yang Berhubungan Dengan Perilaku Penggunaan Alat Kontrasepsi Non Mket Pada Wus Peserta KB Aktif Di Kecamatan Oebobo Kota KupangYulia PritaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- ID Tungau Debu Rumah Di Kelurahan RanotanaDocument5 pagesID Tungau Debu Rumah Di Kelurahan RanotanaYulia PritaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Jurnal 2Document8 pagesJurnal 2Yulia PritaNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Jurnal Musik Pra Oprasi Mengalami Penurunan Kecemasan PDFDocument9 pagesJurnal Musik Pra Oprasi Mengalami Penurunan Kecemasan PDFYulia PritaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Pathophysiology and Treatment Syok Septic in PediatricDocument41 pagesPathophysiology and Treatment Syok Septic in PediatricGustomo PanantroNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- ICU-Acquired Weakness and Recovery From Critical IllnessDocument9 pagesICU-Acquired Weakness and Recovery From Critical IllnessFebrian ParuraNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- A Review of The Outpatient Treatment Methods For COVID-19: A Special Interview With Dr. Pierre KoryDocument41 pagesA Review of The Outpatient Treatment Methods For COVID-19: A Special Interview With Dr. Pierre KoryJan Willem van BorselenNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
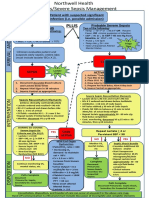
- Patient With Suspected Significant Infection (I.e. Possible Admission)Document2 pagesPatient With Suspected Significant Infection (I.e. Possible Admission)Ryaa Nitaa AdyaaNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Multiple Organ Dysfunction Syndrome in Sepsis: 16 Mei 2016 BackgroundDocument6 pagesMultiple Organ Dysfunction Syndrome in Sepsis: 16 Mei 2016 BackgroundrahayuNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Clinical Case Report Powerpoint PresentationDocument24 pagesClinical Case Report Powerpoint Presentationapi-354139540100% (1)
- Resuscitation Fluids - NEJMDocument9 pagesResuscitation Fluids - NEJMJHWNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Severe Sepsisand Septic Shock GuidelinesDocument17 pagesSevere Sepsisand Septic Shock GuidelinesdrquamrulNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Sirs & ModsDocument5 pagesSirs & Modsmarlou agananNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Viarasilpa Et Al 2019 Venous Thromboembolism in Neurocritical Care PatientsDocument9 pagesViarasilpa Et Al 2019 Venous Thromboembolism in Neurocritical Care Patientsateia83No ratings yet
- Guide To The Intercollegiate MRCS Examination - Singapore 2012Document55 pagesGuide To The Intercollegiate MRCS Examination - Singapore 2012juweriyNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- BronchiolitisDocument17 pagesBronchiolitisRizky DarmawanNo ratings yet
- Use of Vasopressors and InotropesDocument16 pagesUse of Vasopressors and InotropesIrving H Torres LopezNo ratings yet
- Erythroderma: Key PointsDocument5 pagesErythroderma: Key Pointsramdani witiaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- HemorrhageDocument239 pagesHemorrhageparmeshori100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- 2012 CHD 3 Annual ReportDocument72 pages2012 CHD 3 Annual Reportjedy_08No ratings yet
- Module 7 - Meningitis and EncephalitisDocument35 pagesModule 7 - Meningitis and EncephalitisRick RanitNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Indications and Hemoglobin Thresholds For Red Blood Cell Transfusion in The Adult - UpToDateDocument39 pagesIndications and Hemoglobin Thresholds For Red Blood Cell Transfusion in The Adult - UpToDateAhmed MostafaNo ratings yet
- Kuliah Syok 2020 (DR Ahmad Yafiz Hasby SpAn)Document48 pagesKuliah Syok 2020 (DR Ahmad Yafiz Hasby SpAn)RezaNo ratings yet
- April 2007 Written Summary EMRAPDocument3 pagesApril 2007 Written Summary EMRAPAshleyNo ratings yet
- Urosepsis: Oleh: DR - Yolan Novia Ulfah Pembimbing: Dr. Prabudi, SP.B (K) Onk, M.Kes, FICSDocument30 pagesUrosepsis: Oleh: DR - Yolan Novia Ulfah Pembimbing: Dr. Prabudi, SP.B (K) Onk, M.Kes, FICSYolan Novia UlfahNo ratings yet
- SIRS, Sepsis, and Septic Shock Criteria - MDCalcDocument4 pagesSIRS, Sepsis, and Septic Shock Criteria - MDCalcMustafa AadanNo ratings yet
- SSC 2021 GuidelinesDocument59 pagesSSC 2021 GuidelinesPrasannakumar P CNo ratings yet
- Novel Tools For Hemodynamic Monitoring in Critically Ill Patients With Shock - UpToDateDocument26 pagesNovel Tools For Hemodynamic Monitoring in Critically Ill Patients With Shock - UpToDateAlex KuliaNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Assessment Diagnosis Planning Nursing Intervention Rationale EvaluationDocument4 pagesAssessment Diagnosis Planning Nursing Intervention Rationale EvaluationJoshua De Guzman MiraNo ratings yet
- Campbell 2006Document9 pagesCampbell 2006Sílvia TrindadeNo ratings yet
- Shock in Obstetrics: Dr. Hem Nath Subedi Resident ObgynDocument25 pagesShock in Obstetrics: Dr. Hem Nath Subedi Resident ObgynNinaNo ratings yet
- Fournier's Gangrene: An Experience in Tertiary Care HospitalDocument9 pagesFournier's Gangrene: An Experience in Tertiary Care HospitalKriti KumariNo ratings yet
- Role of Synthetic Proteins and Peptides in AnimalsDocument7 pagesRole of Synthetic Proteins and Peptides in AnimalsroniNo ratings yet
- Reference Intervals List - Printed Format Version 1 FinalDocument3 pagesReference Intervals List - Printed Format Version 1 FinalShady FawazNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)