You might also like
- IODINE - Solution To HealthproblemsDocument95 pagesIODINE - Solution To Healthproblemshappycamper100% (60)
- Vitamin B17, Known As Laetrile and Amygdalin, Kills CancerDocument2 pagesVitamin B17, Known As Laetrile and Amygdalin, Kills Cancerapi-31496102075% (4)
- Fundamentals of OncologyDocument1,012 pagesFundamentals of Oncologyainie88% (8)
- 8TH Edition TNM Classification and Significance of Depth of InvasionDocument75 pages8TH Edition TNM Classification and Significance of Depth of InvasionDR. ISHITA SINGHAL50% (2)
- How Nations Succeed A Legatum Institute ReportDocument134 pagesHow Nations Succeed A Legatum Institute ReportDr-Rabia AlmamalookNo ratings yet
- 5G What You Need To KnowDocument2 pages5G What You Need To KnowAlex Ness100% (1)
- Documentation of Red Flags by Physical Therapists For Patients With Low Back PainDocument8 pagesDocumentation of Red Flags by Physical Therapists For Patients With Low Back PainBwizerNo ratings yet
- WWS - 1thru46 Wellness WorksheetsDocument110 pagesWWS - 1thru46 Wellness WorksheetsThalia Sanders100% (1)
- FrontDocument24 pagesFrontBEST STREET WORKOUT LCNo ratings yet
- Cancer of LarynxDocument3 pagesCancer of LarynxShreyas WalvekarNo ratings yet
- Day 3 Activity: Nursing Care Plan: College of Health SciencesDocument6 pagesDay 3 Activity: Nursing Care Plan: College of Health SciencesAngelica Charisse BuliganNo ratings yet
- Benign Salivary Gland Tumors - StatPearls - NCBI BookshelfDocument20 pagesBenign Salivary Gland Tumors - StatPearls - NCBI BookshelfMadhura Shekatkar100% (1)
- Smart FactoriesDocument68 pagesSmart FactoriesDr-Rabia AlmamalookNo ratings yet
- No. Gender Birth Date Diagnosis Stage Value1Document9 pagesNo. Gender Birth Date Diagnosis Stage Value1AdNo ratings yet
- Datosej OilDocument11 pagesDatosej OilSergioVillagomezNo ratings yet
- US6513246 Modelo de Utilidad InternacionalDocument11 pagesUS6513246 Modelo de Utilidad InternacionalKevin RomeroNo ratings yet
- Us 5862996Document9 pagesUs 5862996Efabind OtNo ratings yet
- MCA195MOCA20190630NI000826002060C01Document132 pagesMCA195MOCA20190630NI000826002060C01AdrianaNo ratings yet
- 1Document40 pages1ARNOL ELIAN PEREZ PEÑANo ratings yet
- Asset Managers BrewersDocument14 pagesAsset Managers BrewersWIERDMENo ratings yet
- Optometrist MCQDocument8 pagesOptometrist MCQVisionTrust Eyecare OdayanchalNo ratings yet
- 2017-10-06 Data Market IndicesDocument536 pages2017-10-06 Data Market Indicesy.g.thomasNo ratings yet
- Kerala Public Service CommissionDocument76 pagesKerala Public Service CommissionVijisha KNo ratings yet
- Lessons From The 1930s Great DepressionDocument33 pagesLessons From The 1930s Great Depressionasifjagirani47No ratings yet
- 2ND HR MetricsDocument17 pages2ND HR MetricsAakarshan KesarwaniNo ratings yet
- Civil EngineeringDocument18 pagesCivil EngineeringSANTOSHINo ratings yet
- 11 Si Civil PDFDocument2 pages11 Si Civil PDFNeeraj NNo ratings yet
- Karnataka Power Transmission Corporation LimitedDocument3 pagesKarnataka Power Transmission Corporation LimitedPeterGomesNo ratings yet
- United States Patent (19) : 9 (VE Ump F-AsDocument11 pagesUnited States Patent (19) : 9 (VE Ump F-AsaliNo ratings yet
- 5 1 1-Ridf-CurvesDocument18 pages5 1 1-Ridf-Curvesjohn rey toledoNo ratings yet
- Admi Sicci ADocument8 pagesAdmi Sicci AMarina DavidNo ratings yet
- StatusOfTreaties PDFDocument3 pagesStatusOfTreaties PDFbehzad parsiNo ratings yet
- Eva - Estatus de Vacunas Actualizada - Sem 40Document6 pagesEva - Estatus de Vacunas Actualizada - Sem 40SSOMA C&C EVA SACNo ratings yet
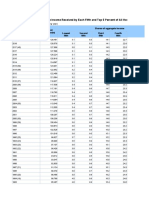
- Table H-2. Share of Aggregate Income Received by Each Fifth and Top 5 Percent of Households, All Races: 1967 To 2014Document9 pagesTable H-2. Share of Aggregate Income Received by Each Fifth and Top 5 Percent of Households, All Races: 1967 To 2014Ola ANo ratings yet
- United States PatentDocument26 pagesUnited States Patentahmad obeidNo ratings yet
- Graficasde CamposDocument6 pagesGraficasde CamposAnonymous Vzdh4qAS0FNo ratings yet
- RL 109Document14 pagesRL 109Passidea TabgNo ratings yet
- Lesson From 1930 2Document33 pagesLesson From 1930 2Wendy GarcíaNo ratings yet
- US5032150Document14 pagesUS5032150MLBB GamingNo ratings yet
- United States Patent (19) : 11) Patent Number: (45) Date of PatentDocument39 pagesUnited States Patent (19) : 11) Patent Number: (45) Date of PatentyasamanNo ratings yet
- Kerala Public Service CommissionDocument7 pagesKerala Public Service CommissionsindhuNo ratings yet
- Anti-Resonance Pipe ClipDocument6 pagesAnti-Resonance Pipe ClipTUNCAY GUMUSNo ratings yet
- Ulllted States Patent (10) Patent N0.: US 8,136,672 B2Document11 pagesUlllted States Patent (10) Patent N0.: US 8,136,672 B2pamururamuNo ratings yet
- Dni Titular As - Nombreas - Sexo As - Fecnac Nombre Tittitular Ipress Celular1Document32 pagesDni Titular As - Nombreas - Sexo As - Fecnac Nombre Tittitular Ipress Celular1Shoron Yosquy Aragon MedranoNo ratings yet
- SA20231226Document11 pagesSA20231226oscarNo ratings yet
- Taylor: United States Patent 19Document15 pagesTaylor: United States Patent 19RoyLoraGallardoNo ratings yet
- Pscnet Lgs 457 18 Kottayam PDFDocument64 pagesPscnet Lgs 457 18 Kottayam PDFGt VinodNo ratings yet
- Patent US4900048ADocument26 pagesPatent US4900048Aabdul bariNo ratings yet
- US5831196 Sensor Assembly For Stringed Musical Instruments PDFDocument10 pagesUS5831196 Sensor Assembly For Stringed Musical Instruments PDFZalNo ratings yet
- United States Patent (10) Patent No.: US 8,747.284 B2Document8 pagesUnited States Patent (10) Patent No.: US 8,747.284 B2Alex MungaiNo ratings yet
- United States Patent (19) : Kaye Oct. 15, 1996Document44 pagesUnited States Patent (19) : Kaye Oct. 15, 1996KrozeNo ratings yet
- United States Patent 19) 11 Patent Number: 5,097,917: Serizawa Et Al. (45) Date of Patent: Mar. 24, 1992Document17 pagesUnited States Patent 19) 11 Patent Number: 5,097,917: Serizawa Et Al. (45) Date of Patent: Mar. 24, 1992priyanka sNo ratings yet
- United States Patent (10) Patent No.: US 6,527,353 B1: Bradfish Et Al. (45) Date of Patent: Mar. 4, 2003Document9 pagesUnited States Patent (10) Patent No.: US 6,527,353 B1: Bradfish Et Al. (45) Date of Patent: Mar. 4, 2003Renato GavanNo ratings yet
- Ati:F:Ht1: Service BulletinDocument42 pagesAti:F:Ht1: Service BulletinJuan Ruben GarciaNo ratings yet
- United States PatentDocument15 pagesUnited States PatentAlexcel CorporalNo ratings yet
- Unlted States Patent (10) Patent N0.2 US 7,417,009 B2Document7 pagesUnlted States Patent (10) Patent N0.2 US 7,417,009 B2Michael MedinaNo ratings yet
- Us5591802 PDFDocument7 pagesUs5591802 PDFAl Saraaf MohammedNo ratings yet
- United States Patent (19) 11 Patent Number: 5,928,426: Aitchison (45) Date of Patent: Jul. 27, 1999Document17 pagesUnited States Patent (19) 11 Patent Number: 5,928,426: Aitchison (45) Date of Patent: Jul. 27, 1999hosseinNo ratings yet
- Santalucia AAADocument52 pagesSantalucia AAAElmer BautistaNo ratings yet
- Censo Enfermedades Cronicas No Transmisibles (Hta) : C/P: DR (A) : Fecha: # Nombre Apellido Edad Sexo CI Fecha N TelefDocument9 pagesCenso Enfermedades Cronicas No Transmisibles (Hta) : C/P: DR (A) : Fecha: # Nombre Apellido Edad Sexo CI Fecha N TelefFlor MarcoNo ratings yet
- DGA of CT OilDocument13 pagesDGA of CT Oilraza239No ratings yet
- US530Document50 pagesUS530wen longNo ratings yet
- US6337429Document14 pagesUS6337429Tasneem MNo ratings yet
- United States Patent (10) Patent No.: US 6,886,777 B2: Rock (45) Date of Patent: May 3, 2005Document24 pagesUnited States Patent (10) Patent No.: US 6,886,777 B2: Rock (45) Date of Patent: May 3, 2005Ionel ConstantinescuNo ratings yet
- 1997 DARPA Funding ListDocument14 pages1997 DARPA Funding Listnipab94816No ratings yet
- United States Patent (19) 11 Patent Number: 5,878,491Document11 pagesUnited States Patent (19) 11 Patent Number: 5,878,491Edmealem Belay MekonnenNo ratings yet
- List of TC - Albay (1948-2018)Document4 pagesList of TC - Albay (1948-2018)Mhio TayamNo ratings yet
- Table H-2. Share of Aggregate Income Received by Each Fifth and Top 5 Percent of All Households: 1967 To 2019Document4 pagesTable H-2. Share of Aggregate Income Received by Each Fifth and Top 5 Percent of All Households: 1967 To 2019DavidNo ratings yet
- 01 Búsquedas EjercicosDocument17 pages01 Búsquedas EjercicosKiara EspinozaNo ratings yet
- CourtwatchnolaDocument32 pagesCourtwatchnolaapi-327999779No ratings yet
- Deep Learning in Smart Grid Technology A Review of Recent Advancements and Future ProspectsDocument21 pagesDeep Learning in Smart Grid Technology A Review of Recent Advancements and Future ProspectsDr-Rabia AlmamalookNo ratings yet
- FY 2021 USAID Journey To Self-Reliance Country Roadmap Methodology GuideDocument50 pagesFY 2021 USAID Journey To Self-Reliance Country Roadmap Methodology GuideDr-Rabia AlmamalookNo ratings yet
- Transformation of Smart Grid Using Machine Learning: November 2019Document7 pagesTransformation of Smart Grid Using Machine Learning: November 2019Dr-Rabia AlmamalookNo ratings yet
- The 2008 Legatum Prosperity Index ReportDocument105 pagesThe 2008 Legatum Prosperity Index ReportDr-Rabia AlmamalookNo ratings yet
- Applsci 11 00237 v3Document28 pagesApplsci 11 00237 v3Dr-Rabia AlmamalookNo ratings yet
- 2018 Prosperity IndexDocument76 pages2018 Prosperity IndexDr-Rabia AlmamalookNo ratings yet
- NAHAERDocument229 pagesNAHAERDr-Rabia AlmamalookNo ratings yet
- StrockeDocument17 pagesStrockeDr-Rabia AlmamalookNo ratings yet
- Hu Dissertation EtdDocument157 pagesHu Dissertation EtdDr-Rabia AlmamalookNo ratings yet
- The Usability Engineering Lifecycle A Case StudyDocument23 pagesThe Usability Engineering Lifecycle A Case StudyDr-Rabia AlmamalookNo ratings yet
- Ada 378838Document288 pagesAda 378838Dr-Rabia AlmamalookNo ratings yet
- Gabbard 2003 HsisDocument13 pagesGabbard 2003 HsisDr-Rabia AlmamalookNo ratings yet
- Usability Evaluation of E-Learning Applications,: A Case Study of It's Learning From A Student's PerspectiveDocument79 pagesUsability Evaluation of E-Learning Applications,: A Case Study of It's Learning From A Student's PerspectiveDr-Rabia AlmamalookNo ratings yet
- Ballard Umn 0130E 11150Document407 pagesBallard Umn 0130E 11150Dr-Rabia AlmamalookNo ratings yet
- Improving Online Course Design Through Usability Testing: Efisher@uab - EduDocument18 pagesImproving Online Course Design Through Usability Testing: Efisher@uab - EduDr-Rabia AlmamalookNo ratings yet
- A I U I M L A S P U ' PDocument16 pagesA I U I M L A S P U ' PDr-Rabia AlmamalookNo ratings yet
- Investigation of Prototype Roles in Conceptual Design Using Case Study and Protocol Study MethodsDocument240 pagesInvestigation of Prototype Roles in Conceptual Design Using Case Study and Protocol Study MethodsDr-Rabia AlmamalookNo ratings yet
- Myx 1Document143 pagesMyx 1Dr-Rabia AlmamalookNo ratings yet
- Applied Radiation Oncology: Case Report: Strip Alopecia in High-Dose VMAT-based Stereotactic RadiosurgeryDocument4 pagesApplied Radiation Oncology: Case Report: Strip Alopecia in High-Dose VMAT-based Stereotactic RadiosurgeryBiplab SarkarNo ratings yet
- Cancer Nursing Management: Study Online atDocument3 pagesCancer Nursing Management: Study Online atLilly DayeNo ratings yet
- Breast CancerDocument18 pagesBreast CancerJohn AlcantaraNo ratings yet
- Viewcontent CgiDocument92 pagesViewcontent CgiDhananjai YadavNo ratings yet
- Amoora RohitukaDocument3 pagesAmoora Rohitukamadhavkrishna gargNo ratings yet
- Cost of Treatment For Cancer Experiences of PatienDocument7 pagesCost of Treatment For Cancer Experiences of PatienSanoj MaveliNo ratings yet
- MCQs EPIDEMIOLOGY BLOCK 1 REVISION 2020Document33 pagesMCQs EPIDEMIOLOGY BLOCK 1 REVISION 2020spitzmark2030No ratings yet
- The Orgone Accumulator Handbook WilhelmDocument19 pagesThe Orgone Accumulator Handbook WilhelmKamal HaasanNo ratings yet
- LS7B Week 3 Lectures Slides STUDENTSDocument78 pagesLS7B Week 3 Lectures Slides STUDENTSSoji AdimulaNo ratings yet
- Li v. Soliman-DigestDocument3 pagesLi v. Soliman-DigestEloisa SalitreroNo ratings yet
- K7 Genetic Counseling-2021Document30 pagesK7 Genetic Counseling-2021felixNo ratings yet
- Osteosarcoma DR: Gehan MohamedDocument19 pagesOsteosarcoma DR: Gehan MohamedNico DougaNo ratings yet
- Immunodiagnosis and Immunotherapy of Infections (Amb 710)Document33 pagesImmunodiagnosis and Immunotherapy of Infections (Amb 710)CHINEDU CHUKWUBIKE0% (1)
- Parham, Barbara-What's Wrong With Eating Meat - Ananda Marga Publications (1979) PDFDocument11 pagesParham, Barbara-What's Wrong With Eating Meat - Ananda Marga Publications (1979) PDFDharmaMaya ChandrahasNo ratings yet
- READINGDocument21 pagesREADINGdiya baby100% (1)
- Biology Project Report Class 12 Cbse 2020-2021 On On Topic CancerDocument10 pagesBiology Project Report Class 12 Cbse 2020-2021 On On Topic CancerNIKHIL SINGH100% (1)
- Cjim 12 573Document7 pagesCjim 12 573MR Emam - GamingNo ratings yet
- Prostate CarcinomaDocument42 pagesProstate CarcinomaWhydia Wedha SutedjaNo ratings yet
- Closing The Cancer Divide: A Blueprint For ActionDocument45 pagesClosing The Cancer Divide: A Blueprint For ActionPresentaciones_FKNo ratings yet
- 3.1.5.A SecretsInGenesDocument6 pages3.1.5.A SecretsInGenesSumukh ChandaNo ratings yet