You might also like
- House OfficerDocument32 pagesHouse Officerapi-3705046100% (1)
- HydronephrosisDocument3 pagesHydronephrosisCarla AlmerolNo ratings yet
- Pi Is 2210261215001479Document3 pagesPi Is 2210261215001479hussein_faourNo ratings yet
- Complex Case of Ureteropelvic Junction Obstruction 2024 International JournaDocument3 pagesComplex Case of Ureteropelvic Junction Obstruction 2024 International JournaRonald QuezadaNo ratings yet
- Use of locking-loop nephrostomy catheters in dogs and catsDocument10 pagesUse of locking-loop nephrostomy catheters in dogs and catsBernardo BertoldiNo ratings yet
- Organ Transplantation Historial Perspective and Current PracticeDocument14 pagesOrgan Transplantation Historial Perspective and Current PracticehkdawnwongNo ratings yet
- Renal Replacement Therapy Review: Past, Present and FutureDocument11 pagesRenal Replacement Therapy Review: Past, Present and FuturerkNo ratings yet
- Anomalous Non-bifurcating Portal Vein Protected During Extended Right Hepatectomy Using Hanging ManeuverDocument7 pagesAnomalous Non-bifurcating Portal Vein Protected During Extended Right Hepatectomy Using Hanging ManeuverMARIO DCARLO TREJO HUAMANNo ratings yet
- Pearse Et Al 2018 Non Functioning KidneyDocument4 pagesPearse Et Al 2018 Non Functioning Kidneyabdalsalaam1No ratings yet
- Article 39794Document4 pagesArticle 39794d.amouzou1965No ratings yet
- Correspondence To EditorDocument2 pagesCorrespondence To Editormanfel_26No ratings yet
- Yan 2015Document4 pagesYan 2015ELIECERNo ratings yet
- Transplantation of Organs Feasible or Practical?: Wizen IsDocument32 pagesTransplantation of Organs Feasible or Practical?: Wizen IswunderfullifeNo ratings yet
- Bile Leak CaseDocument6 pagesBile Leak CaseDimas ErlanggaNo ratings yet
- Retroperitoneal Appendicitis: A Surgical Dilemma: Euroasian Journal of Hepato-Gastroenterology January 2013Document3 pagesRetroperitoneal Appendicitis: A Surgical Dilemma: Euroasian Journal of Hepato-Gastroenterology January 2013putraNo ratings yet
- Percutaneous Nephrolithotomy in Case of Crossed Fused Renal Ectopia: A Case ReportDocument3 pagesPercutaneous Nephrolithotomy in Case of Crossed Fused Renal Ectopia: A Case ReportDr.ankit AnandNo ratings yet
- Historical Article: The First Human Renal TransplantsDocument3 pagesHistorical Article: The First Human Renal TransplantsRossalia VisserNo ratings yet
- Subsidence of Hypertension in A Patient With GiantDocument4 pagesSubsidence of Hypertension in A Patient With GiantSinbijeo GinNo ratings yet
- Comparison of Open and Laproscopic Live Donor NephrectomyDocument7 pagesComparison of Open and Laproscopic Live Donor NephrectomyEhab Omar El HalawanyNo ratings yet
- 804 FullDocument8 pages804 FullNoor HadyNo ratings yet
- JOURNALDocument4 pagesJOURNALChiara FajardoNo ratings yet
- Severe Pelvic Fracture With Profound Hypotension: A Case Report and Treatment AlgorithmDocument3 pagesSevere Pelvic Fracture With Profound Hypotension: A Case Report and Treatment AlgorithmodyNo ratings yet
- 2018 Article 1089Document5 pages2018 Article 1089Andreea StreuleaNo ratings yet
- Fistula Nefrocolica Por RFADocument3 pagesFistula Nefrocolica Por RFARenan DiasNo ratings yet
- Reconstruction of Late-Onset Transplant Ureteral Stricture DiseaseDocument6 pagesReconstruction of Late-Onset Transplant Ureteral Stricture DiseaseAnanda KumarNo ratings yet
- Ureteric ComplicationsDocument7 pagesUreteric ComplicationstnsourceNo ratings yet
- Borges Dias 2016Document2 pagesBorges Dias 2016Fandi AhmadNo ratings yet
- Yu 2013Document4 pagesYu 2013raissametasariNo ratings yet
- Hepatic Subcapsular BIloma A Rare Complication of Laparoscopic CholecystectomyDocument4 pagesHepatic Subcapsular BIloma A Rare Complication of Laparoscopic CholecystectomyIndra PrimaNo ratings yet
- Metro Fan ofDocument3 pagesMetro Fan ofsahandNo ratings yet
- Management of Penile Fracture: Ahmad M. El-Taher, Hassan A. Aboul-Ella, Mohamed A. Sayed, and Atef A. GaafarDocument3 pagesManagement of Penile Fracture: Ahmad M. El-Taher, Hassan A. Aboul-Ella, Mohamed A. Sayed, and Atef A. GaafarTeja LaksanaNo ratings yet
- Use of The Appendix To Replace A Ureter. Case ReportDocument2 pagesUse of The Appendix To Replace A Ureter. Case ReportPacVitorNo ratings yet
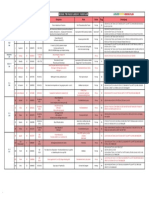
- Timetable PosterExDocument45 pagesTimetable PosterExNeo Rodriguez AlvaradoNo ratings yet
- Retroperitoneal Appendicitis: A Surgical DilemmaDocument2 pagesRetroperitoneal Appendicitis: A Surgical DilemmaputraNo ratings yet
- Portocaval Shunt Throughout Anhepatic Phase in Orthotopic Liver Transplantation For Cirrhotic PatientsDocument5 pagesPortocaval Shunt Throughout Anhepatic Phase in Orthotopic Liver Transplantation For Cirrhotic PatientsHưng Nguyễn KiềuNo ratings yet
- Ureteroneocystostomy For Treatment of Struvite UroDocument4 pagesUreteroneocystostomy For Treatment of Struvite UroBright DerlacuzENo ratings yet
- PDF PreviewDocument9 pagesPDF PreviewSowmya ChitraNo ratings yet
- Wunderlich Syndrome Spontaneous Atraumatic Rupture of The KidneyDocument5 pagesWunderlich Syndrome Spontaneous Atraumatic Rupture of The KidneyqalbiNo ratings yet
- Nasser2015Document5 pagesNasser2015hengkileonardNo ratings yet
- Cirugi A Espan Ola: Meso-Cava Bypass As An Alternative To Multivisceral TransplantationDocument2 pagesCirugi A Espan Ola: Meso-Cava Bypass As An Alternative To Multivisceral TransplantationHưng Nguyễn KiềuNo ratings yet
- Ahn 2011Document4 pagesAhn 2011Residentes PediatríaNo ratings yet
- Complications of Percutaneous Nephrostomy Tube Placement To Treat NephrolithiasisDocument4 pagesComplications of Percutaneous Nephrostomy Tube Placement To Treat NephrolithiasisPande Made FitawijamariNo ratings yet
- Marion 2020Document7 pagesMarion 2020hezzaNo ratings yet
- Abdominopelvic Ectopic Spleen With A Comprehensive Imaging Examination: A Case ReportDocument6 pagesAbdominopelvic Ectopic Spleen With A Comprehensive Imaging Examination: A Case ReportceciliaNo ratings yet
- BRIEF CLINICAL OBSERVATIONS: Nondilated Obstructive Uropathy Due to a Ureteral CalculusDocument3 pagesBRIEF CLINICAL OBSERVATIONS: Nondilated Obstructive Uropathy Due to a Ureteral CalculusMuhammad Kholid FirdausNo ratings yet
- IVC Leiomyosarcoma Reconstruction Not Always RequiredDocument3 pagesIVC Leiomyosarcoma Reconstruction Not Always RequiredCirugía General Hospital de San JoséNo ratings yet
- Case Report Severe Dysplasia of Kidney 20082021Document15 pagesCase Report Severe Dysplasia of Kidney 20082021Nikko Caesario Mauldy SusiloNo ratings yet
- Trauma UretraDocument3 pagesTrauma UretraTita FadiahNo ratings yet
- Pediatric Bladder Injuries from Inguinal Canal SurgeryDocument4 pagesPediatric Bladder Injuries from Inguinal Canal SurgeryOscar Sanchez ParisNo ratings yet
- Review Syefira SalshabilaDocument2 pagesReview Syefira Salshabilaqueen TinaNo ratings yet
- Outcome of Septal Dermoplasty in Patients With Hereditary Hemorrhagic TelangiectasiaDocument5 pagesOutcome of Septal Dermoplasty in Patients With Hereditary Hemorrhagic TelangiectasiaalecsaNo ratings yet
- Crossed and Non-Fused Renal Ectopia of Inferior Type: G. J. Jorwekar, K. N. Dandekar, R. K. Shinde, P. K. BaviskarDocument3 pagesCrossed and Non-Fused Renal Ectopia of Inferior Type: G. J. Jorwekar, K. N. Dandekar, R. K. Shinde, P. K. BaviskarnaseebulNo ratings yet
- Total Laparoscopic Duodenopancreatectomy Case ReportDocument7 pagesTotal Laparoscopic Duodenopancreatectomy Case ReportIJAR JOURNALNo ratings yet
- Complication of Long Indwelling Urinary Catheter and StentDocument5 pagesComplication of Long Indwelling Urinary Catheter and StenteviltohuntNo ratings yet
- Undescended TestisDocument3 pagesUndescended TestisIoannis ValioulisNo ratings yet
- Jiang2018 2Document5 pagesJiang2018 2Anonymous Inj7eQNo ratings yet
- JCDR 9 PD26Document2 pagesJCDR 9 PD26ceciliaNo ratings yet
- 1 s2.0 S0022480423002895 MainDocument7 pages1 s2.0 S0022480423002895 Mainlucabarbato23No ratings yet
- Reconstruction of Late-Onset Transplant Ureteral Stricture DiseaseDocument7 pagesReconstruction of Late-Onset Transplant Ureteral Stricture DiseasetnsourceNo ratings yet
- Testicular Torsion in Undescended TestisDocument5 pagesTesticular Torsion in Undescended TestisjimNo ratings yet
- 279 285 1 SM PDFDocument6 pages279 285 1 SM PDFLainatussifah QamalNo ratings yet
- Quotation Letter Onkologi in Nov - Dec 2019-1Document4 pagesQuotation Letter Onkologi in Nov - Dec 2019-1Ikhdin SaadhiNo ratings yet
- Clinical Pathways for Rib FractureDocument1 pageClinical Pathways for Rib FractureIkhdin SaadhiNo ratings yet
- +++pappachan-Biomekanik MF Trauma PDFDocument7 pages+++pappachan-Biomekanik MF Trauma PDFmedicamedicaNo ratings yet
- Pain Management & Medicine: An Innovative Product For Pain Management: Proof From Clinical TrialDocument5 pagesPain Management & Medicine: An Innovative Product For Pain Management: Proof From Clinical TrialIkhdin SaadhiNo ratings yet
- Akomodasi SSF Rev6Document28 pagesAkomodasi SSF Rev6Ikhdin Saadhi0% (1)
- E019614 FullDocument7 pagesE019614 FullIkhdin SaadhiNo ratings yet
- Anggrek 1: Ruang PJ BED Nama Usia RM MRS Diagnosis Status Plan DPJP KeteranganDocument2 pagesAnggrek 1: Ruang PJ BED Nama Usia RM MRS Diagnosis Status Plan DPJP KeteranganIkhdin SaadhiNo ratings yet
- BTKV MappingDocument1 pageBTKV MappingIkhdin SaadhiNo ratings yet
- Traumatic Brain Injury and Treatment With Hypertonic Sodium Lactate. Will It Become The Best Management Alternative?Document15 pagesTraumatic Brain Injury and Treatment With Hypertonic Sodium Lactate. Will It Become The Best Management Alternative?Ikhdin SaadhiNo ratings yet
- 11 11 18-2Document4 pages11 11 18-2Ikhdin SaadhiNo ratings yet
- Neurofibromatosis Type I (NF1) : Presented by Lei DuDocument18 pagesNeurofibromatosis Type I (NF1) : Presented by Lei DuIkhdin SaadhiNo ratings yet
- Paper I Operative ConsultationDocument64 pagesPaper I Operative ConsultationIkhdin SaadhiNo ratings yet
- Vesicoureteral Reflux 508Document8 pagesVesicoureteral Reflux 508Ikhdin SaadhiNo ratings yet
- Ann Burns and Fire Disasters 27 209Document6 pagesAnn Burns and Fire Disasters 27 209Ikhdin SaadhiNo ratings yet
- Hirsch Pung SDocument10 pagesHirsch Pung Sotto naftariNo ratings yet
- CRG 0011 0755Document8 pagesCRG 0011 0755Ikhdin SaadhiNo ratings yet
- DSV Serial CaseDocument5 pagesDSV Serial CaseIkhdin SaadhiNo ratings yet
- VP ShuntDocument12 pagesVP ShuntBanni Aprilita PratiwiNo ratings yet
- AppendixDocument21 pagesAppendixIkhdin SaadhiNo ratings yet
- SICH Mgmt2Document9 pagesSICH Mgmt2Lennon Ponta-oyNo ratings yet
- 1501931700998Document26 pages1501931700998Ikhdin SaadhiNo ratings yet
- Neu 2014 3644Document12 pagesNeu 2014 3644Ikhdin SaadhiNo ratings yet
- 1501931700998Document26 pages1501931700998Ikhdin SaadhiNo ratings yet
- Ni Hms 865156Document8 pagesNi Hms 865156Ikhdin SaadhiNo ratings yet
- AppendixDocument21 pagesAppendixIkhdin SaadhiNo ratings yet
- Pi Is 0741521402753214Document3 pagesPi Is 0741521402753214Ikhdin SaadhiNo ratings yet
- L - GS PM 021415 Cohn PercutDocument9 pagesL - GS PM 021415 Cohn PercutIkhdin SaadhiNo ratings yet
- JSurgTechCaseReport411-2985968 081739Document5 pagesJSurgTechCaseReport411-2985968 081739Ikhdin SaadhiNo ratings yet
- Memory in AutismDocument384 pagesMemory in AutismkapsicumNo ratings yet
- Diacalauto en DT Rev03 0851501 Rev02Document8 pagesDiacalauto en DT Rev03 0851501 Rev02vijayramaswamy0% (1)
- Dexmedetomidine FAQDocument16 pagesDexmedetomidine FAQRoxana SurliuNo ratings yet
- Adult Early Warning Score Observation Chart For Cardiothoracic UnitDocument1 pageAdult Early Warning Score Observation Chart For Cardiothoracic UnitalexipsNo ratings yet
- Health Entrepreneurship in PakistanDocument44 pagesHealth Entrepreneurship in Pakistanusman-hbNo ratings yet
- Medical Mycology GuideDocument39 pagesMedical Mycology Guidehanny jammyNo ratings yet
- Yimi Catalogue2014Document60 pagesYimi Catalogue2014ariovaldofjNo ratings yet
- Assessing The Caring Behaviors of Critical Care Nurses PDFDocument9 pagesAssessing The Caring Behaviors of Critical Care Nurses PDFnasimhsNo ratings yet
- MiradryDocument4 pagesMiradryBarakat AyoubNo ratings yet
- Biology Terms Grade 9 ReviewerDocument3 pagesBiology Terms Grade 9 ReviewerGreta Uy Sevilla100% (1)
- The Pittston Dispatch 08-05-2012Document62 pagesThe Pittston Dispatch 08-05-2012The Times LeaderNo ratings yet
- 1891 Knowles Complete System of Personal InfluenceDocument154 pages1891 Knowles Complete System of Personal InfluenceJoão Marques Ferreira100% (3)
- Newborn Care Charts Guide Routine Care and ManagementDocument102 pagesNewborn Care Charts Guide Routine Care and ManagementM. KurnNo ratings yet
- Anatomy StomachDocument43 pagesAnatomy StomachBijo K BennyNo ratings yet
- Slide 11 DiagimgDocument39 pagesSlide 11 Diagimghayumbe08No ratings yet
- Teaching Practice.... Lung CancerDocument32 pagesTeaching Practice.... Lung CancernamitaNo ratings yet
- Estudo Hepasfera Versus BeadDocument6 pagesEstudo Hepasfera Versus BeadAlexandre Campos Moraes AmatoNo ratings yet
- Christa Maki Letter of Recommednation 4Document2 pagesChrista Maki Letter of Recommednation 4api-491578633No ratings yet
- English 7 1stQ ExamDocument5 pagesEnglish 7 1stQ ExamNoble MartinusNo ratings yet
- Jhonston Evaluation of Growth in Patients Belonging PetrovicsDocument12 pagesJhonston Evaluation of Growth in Patients Belonging PetrovicsMargarida Maria LealNo ratings yet
- GCSE Biology RevisionDocument2 pagesGCSE Biology RevisionsannnnnNo ratings yet
- Cupping The Great Missing Therapy (Dr. Sahbaa M. Bondok)Document240 pagesCupping The Great Missing Therapy (Dr. Sahbaa M. Bondok)Teerth KrishnanandNo ratings yet
- Click Here To Download Top 100 One Word Substitution As PDF FormatDocument3 pagesClick Here To Download Top 100 One Word Substitution As PDF FormatMrinmoy KoleyNo ratings yet
- Abdominal Distention inDocument45 pagesAbdominal Distention inArif Rahman DmNo ratings yet
- Gestational Diabetes Screening Case StudiesDocument50 pagesGestational Diabetes Screening Case Studiesdiabetes asia100% (1)
- Cost-Benefit Analysis Lesson PlanDocument2 pagesCost-Benefit Analysis Lesson PlanlaurahelenkingNo ratings yet
- Is There A Clinical Difference Between Salt Water and Fresh Water DrowningDocument2 pagesIs There A Clinical Difference Between Salt Water and Fresh Water DrowningSicilia Bunga Athifah ArnurNo ratings yet
- Herbst Appliance GuideDocument161 pagesHerbst Appliance GuideRajshekhar Banerjee100% (3)
- Shree Hospital: Bidar CT Scan Bidar CT Scan Bidar CT ScanDocument8 pagesShree Hospital: Bidar CT Scan Bidar CT Scan Bidar CT ScanhattisanjayNo ratings yet