You might also like
- David Deida - Wild NightsDocument120 pagesDavid Deida - Wild NightsRosatvision100% (8)
- Past Life Returner - 01Document309 pagesPast Life Returner - 01Edgar Estebam Soto EstrellaNo ratings yet
- Test Bank For Adolescence 11th Edition by SteinbergDocument23 pagesTest Bank For Adolescence 11th Edition by SteinbergNancy Medez100% (35)
- Health: Quarter 1-Module 6Document25 pagesHealth: Quarter 1-Module 6Niko Igie Albino Pujeda0% (1)
- Ethical Analysis of Dominos Limited Pizza Delivery Policy Working VersionDocument11 pagesEthical Analysis of Dominos Limited Pizza Delivery Policy Working Versionapi-502151650No ratings yet
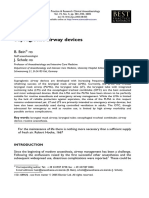
- The Evolution of Airway Management - New Concepts and Conflicts With Traditional PracticeDocument13 pagesThe Evolution of Airway Management - New Concepts and Conflicts With Traditional PracticeKartika RahmawatiNo ratings yet
- Dispositivos - Supragloticos LECTURADocument13 pagesDispositivos - Supragloticos LECTURAAinhoa Jimenez TraperoNo ratings yet
- Hartley 2000Document8 pagesHartley 2000canndy202No ratings yet
- Cover Note: The Evolution of The Rubber Endotracheal TubeDocument2 pagesCover Note: The Evolution of The Rubber Endotracheal TubeerniNo ratings yet
- A Comparison of The Impact of Cuffed Versus.3Document8 pagesA Comparison of The Impact of Cuffed Versus.3SeveNNo ratings yet
- Ojanes 2019121113522570 PDFDocument6 pagesOjanes 2019121113522570 PDFArifudin Cipto HusodoNo ratings yet
- The Evolution of Airway Management - New Concepts and Conflicts With Traditional PracticeDocument13 pagesThe Evolution of Airway Management - New Concepts and Conflicts With Traditional Practicecaca100% (1)
- Aapm 07 02 38899Document4 pagesAapm 07 02 38899NailaIzzethNo ratings yet
- 1 s2.0 S0007091217425281 MainDocument5 pages1 s2.0 S0007091217425281 Mainmanolo.mendozavNo ratings yet
- Baska MaskDocument8 pagesBaska MaskAnish H DaveNo ratings yet
- Cleft Lip and Palate Primary RepairDocument349 pagesCleft Lip and Palate Primary RepairDaiana Opris100% (1)
- Management of The Artificial AirwaDocument17 pagesManagement of The Artificial AirwaGuillermoAlphonsoVasquezGiglioNo ratings yet
- Endotracheal TubeDocument16 pagesEndotracheal TubeArsil RadiansyahNo ratings yet
- Craniofacial Distraction 2017Document234 pagesCraniofacial Distraction 2017Omar VillamizarNo ratings yet
- Laryngeal Mask: Is It The Best Supraglottic Airway?Document12 pagesLaryngeal Mask: Is It The Best Supraglottic Airway?Dr. T. BalasubramanianNo ratings yet
- Pediatric Cuffed Endotracheal TubesDocument6 pagesPediatric Cuffed Endotracheal TubeslakhwinderNo ratings yet
- Laryngeal Mask Airway and Its Variants: Dr. Jayashree SoodDocument6 pagesLaryngeal Mask Airway and Its Variants: Dr. Jayashree SoodParama DinaNo ratings yet
- OJOLNS-10 - II - Invited Editorial PDFDocument5 pagesOJOLNS-10 - II - Invited Editorial PDFDR K C MALLIKNo ratings yet
- Eustachian TubeDocument6 pagesEustachian TubeMusyfiqoh TusholehahNo ratings yet
- ESSE Primary Palatoplasty Using Bipedicle Flaps Modified Von Langenbeck TechniqueDocument10 pagesESSE Primary Palatoplasty Using Bipedicle Flaps Modified Von Langenbeck TechniqueAndre Luis CostaNo ratings yet
- Evolvingmaterials Andtechniquesfor Endoscopicsinus SurgeryDocument20 pagesEvolvingmaterials Andtechniquesfor Endoscopicsinus Surgerydisk_la_poduNo ratings yet
- Surgical Correction Subglottic Stenosis of The Larynx: AnnoldDocument6 pagesSurgical Correction Subglottic Stenosis of The Larynx: Annoldcanndy202No ratings yet
- Recent Research Findings: Management of Open Pneumothorax in The Tactical EnvironmentDocument1 pageRecent Research Findings: Management of Open Pneumothorax in The Tactical EnvironmentToon ToonannNo ratings yet
- What Makes The Pediatric Airway So Diffi Cult?: Jerrold Lerman MD, FRCPC, FANZCADocument3 pagesWhat Makes The Pediatric Airway So Diffi Cult?: Jerrold Lerman MD, FRCPC, FANZCAhugo roblesNo ratings yet
- What Makes The Pediatric Airway So Diffi Cult?: Jerrold Lerman MD, FRCPC, FANZCADocument3 pagesWhat Makes The Pediatric Airway So Diffi Cult?: Jerrold Lerman MD, FRCPC, FANZCAhugo roblesNo ratings yet
- Face Mask Ventilation in Edentulous Patients: A Comparison of Mandibular Groove and Lower Lip PlacementDocument4 pagesFace Mask Ventilation in Edentulous Patients: A Comparison of Mandibular Groove and Lower Lip PlacementLinda Wahyu UtamiiNo ratings yet
- Airway Management - Supraglottic Airway PDFDocument4 pagesAirway Management - Supraglottic Airway PDFPiet Pogen PoelNo ratings yet
- Chapter 4 - Surgery For Choanal Atresia: Eugene N. MyersDocument4 pagesChapter 4 - Surgery For Choanal Atresia: Eugene N. MyersGloriaCorredorNo ratings yet
- Comparation Rubber Dam SistemDocument8 pagesComparation Rubber Dam SistemLiz Stephany GaviriaNo ratings yet
- Otoplasty Through Ventral Skin Incision and Shaping of The Antihelix by Abrasion-A Retrospective StudyDocument8 pagesOtoplasty Through Ventral Skin Incision and Shaping of The Antihelix by Abrasion-A Retrospective StudyKihyun YooNo ratings yet
- Dr. Vernon Coleman - Masks and Mask Wearing - 100 Facts You Must Know - World Doctors AllianceDocument17 pagesDr. Vernon Coleman - Masks and Mask Wearing - 100 Facts You Must Know - World Doctors Alliancejamestahara95No ratings yet
- Objective Assessment of Increase in Breathing Resistance of N95 Respirators On Human SubjectsDocument5 pagesObjective Assessment of Increase in Breathing Resistance of N95 Respirators On Human SubjectsgrowlingtoyouNo ratings yet
- Type of Intubation Tube in Operation Theater 2Document67 pagesType of Intubation Tube in Operation Theater 2Aslah NabilahNo ratings yet
- Artigo 5Document8 pagesArtigo 5doctorbanNo ratings yet
- Optimal Size Selection of The Classic Laryngeal Mask Airway by Tongue Width-Based Method in Male AdultsDocument4 pagesOptimal Size Selection of The Classic Laryngeal Mask Airway by Tongue Width-Based Method in Male AdultsDefayudina Dafilianty RosatariaNo ratings yet
- 4465 15o0tp6 PDFDocument4 pages4465 15o0tp6 PDFahmedbilalakhtar20No ratings yet
- Cannula Versus Needle in Medical Rhinoplasty - The Nose KnowsDocument24 pagesCannula Versus Needle in Medical Rhinoplasty - The Nose KnowsKerlida SantosNo ratings yet
- An Alternative Alar Cinch Suture PDFDocument11 pagesAn Alternative Alar Cinch Suture PDFmatias112No ratings yet
- Pulmonary: Treatment ofDocument5 pagesPulmonary: Treatment ofYantoNo ratings yet
- Fibreoptic Intubation Modern Clinical Practice (2008)Document6 pagesFibreoptic Intubation Modern Clinical Practice (2008)enriquegarciagalianaNo ratings yet
- Surgical Techniques in Cochlear ImplantDocument12 pagesSurgical Techniques in Cochlear Implantretribution499No ratings yet
- Airway Adjuncts 2Document9 pagesAirway Adjuncts 2Paul ButlerNo ratings yet
- Difficult Airway ManagementDocument79 pagesDifficult Airway Managementedwardjohnson2310No ratings yet
- Pediatric Protrusion Mentioned,: Robert M.D. CityDocument2 pagesPediatric Protrusion Mentioned,: Robert M.D. Citybouchra8blsNo ratings yet
- Strengthsandlimitations Ofairwaytechniques: Richard M. CooperDocument15 pagesStrengthsandlimitations Ofairwaytechniques: Richard M. CooperJEFFERSON MUÑOZNo ratings yet
- - اطلس جهاز التخدير-30-34Document5 pages- اطلس جهاز التخدير-30-34علي الاسديNo ratings yet
- s-0034-1395500 BrochotrainerDocument10 pagess-0034-1395500 BrochotraineririsNo ratings yet
- Hong 2005Document13 pagesHong 2005Otto DogNo ratings yet
- Tracheostomy OverviewDocument9 pagesTracheostomy Overview8pvz96ktd9No ratings yet
- Total Lower Lip and Chin Reconstruction With The Free Radial Forearm FlapDocument10 pagesTotal Lower Lip and Chin Reconstruction With The Free Radial Forearm FlapJelihovschi IonNo ratings yet
- Macintosh Laryngoscope I-View and C-MACR Video LarDocument11 pagesMacintosh Laryngoscope I-View and C-MACR Video LarzakyNo ratings yet
- Pediatric Supraglottic Airway DevicesDocument11 pagesPediatric Supraglottic Airway DevicesJyothi VhNo ratings yet
- A Hollow Delayed Surgical ObturatorDocument55 pagesA Hollow Delayed Surgical ObturatorvinnycoolbuddyNo ratings yet
- Microleakage: Apical Seal Vs Coronal Seal: 10.5005/jp-Journals-10015-1215Document4 pagesMicroleakage: Apical Seal Vs Coronal Seal: 10.5005/jp-Journals-10015-1215fridafardanilaNo ratings yet
- Mastoidectomy Intact Canal Wall ProcedureDocument13 pagesMastoidectomy Intact Canal Wall Proceduretaquiri12No ratings yet
- A Brief Chronological Review of Dental Implant HistoryDocument4 pagesA Brief Chronological Review of Dental Implant HistoryJorge SaenzNo ratings yet
- Congress Auricular Reconstruction AbstractsDocument92 pagesCongress Auricular Reconstruction AbstractsRocio RamirezNo ratings yet
- Maxilectomia TotalDocument18 pagesMaxilectomia TotalmonitosmaxilosNo ratings yet
- A Method To Control EpistaxisDocument2 pagesA Method To Control EpistaxisElena TroiaNo ratings yet
- Personality Development NSTPDocument34 pagesPersonality Development NSTPMc HarrisNo ratings yet
- LIC Health Plus Plan No.901 Full FormDocument15 pagesLIC Health Plus Plan No.901 Full FormDhaval SarvaiyaNo ratings yet
- Lucknow University IMS MBA (Marketing) Human Resource ManagementDocument12 pagesLucknow University IMS MBA (Marketing) Human Resource ManagementShadaab AlamNo ratings yet
- (123doc) - Opthalmic-Microsurgical-Suturing-Techniques-Part-3-PpsxDocument15 pages(123doc) - Opthalmic-Microsurgical-Suturing-Techniques-Part-3-PpsxTEODORA MIHAELA PELEASANo ratings yet
- Diet Nutrition & Obesity PreventionDocument50 pagesDiet Nutrition & Obesity Preventionnaina bhangeNo ratings yet
- Resume - Randa MolyneauxDocument1 pageResume - Randa Molyneauxapi-588960966No ratings yet
- The Current Status of Clinical PsychologyDocument35 pagesThe Current Status of Clinical Psychologying. Diosiris CamachoNo ratings yet
- Part E Course Outcomes Assessment Plan: Philippine College of Science and TechnologyDocument2 pagesPart E Course Outcomes Assessment Plan: Philippine College of Science and TechnologyRhona Mae SebastianNo ratings yet
- Chakra Mantra MagickDocument36 pagesChakra Mantra MagickPaul Asturbiaris100% (4)
- Đề Ôn HN 1Document4 pagesĐề Ôn HN 1Tran Thi ThanhNo ratings yet
- Grade9 STE Con.-Chem. Q4 Module-5 Wk6 ADMDocument20 pagesGrade9 STE Con.-Chem. Q4 Module-5 Wk6 ADMChelzy Catabas100% (1)
- AND Extracts Produce Organic Concoction: Prepared By: Marivic A. NeridoDocument37 pagesAND Extracts Produce Organic Concoction: Prepared By: Marivic A. Neridoallen paulo repollo100% (1)
- LastDocument16 pagesLastMira Lei MarigmenNo ratings yet
- Factor Analysis and Construct Validity of The Safer-Home: Teresa Chiu, Rosemary OliverDocument11 pagesFactor Analysis and Construct Validity of The Safer-Home: Teresa Chiu, Rosemary OliverSze Wing LeeNo ratings yet
- Soundarya LahiriDocument50 pagesSoundarya Lahirivsh101No ratings yet
- 8STA AS Motorsport Connector Accessories Catalogue 2022Document11 pages8STA AS Motorsport Connector Accessories Catalogue 2022martin garciaNo ratings yet
- Asthma - Discharge Care For Adults - EnglishDocument2 pagesAsthma - Discharge Care For Adults - EnglishMalik Khuram ShazadNo ratings yet
- Final Project (Community Nutrition)Document21 pagesFinal Project (Community Nutrition)laiba.akhtarNo ratings yet
- QW-Performance Review TemplatesDocument19 pagesQW-Performance Review TemplatesLaksana Anugrah PutraNo ratings yet
- Effect of SnailDocument13 pagesEffect of SnailElvy ChardilaNo ratings yet
- Nutritional AssessmentDocument4 pagesNutritional Assessmentchindobr8No ratings yet
- Vitiligo Fitz PDFDocument51 pagesVitiligo Fitz PDFAbdur RachmanNo ratings yet
- Nutrition Across The LifespanDocument6 pagesNutrition Across The LifespanYuuki Chitose (tai-kun)No ratings yet
- Maintenance ManualDocument12 pagesMaintenance ManualAndrewMeyerNo ratings yet
- Pharmacon Poster 2021Document1 pagePharmacon Poster 2021api-592676308No ratings yet