You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- How To Become A Doctor in The PhilippinesDocument9 pagesHow To Become A Doctor in The PhilippinesLoeyNo ratings yet
- 1) Engage Lgus and Local Stakeholders To Support Province and City-Wide Health Systems IntegrationDocument35 pages1) Engage Lgus and Local Stakeholders To Support Province and City-Wide Health Systems IntegrationEunice MoiraNo ratings yet
- Critical Appraisal WorksheetsDocument10 pagesCritical Appraisal WorksheetsHotmann XtinusNo ratings yet
- Human Relations in NursingDocument15 pagesHuman Relations in NursingOm VaishNav100% (1)
- IJHIM 6 - Nur Husnina (36 SD 42)Document7 pagesIJHIM 6 - Nur Husnina (36 SD 42)RSU Sayang BundaNo ratings yet
- Antropologi PesisirDocument9 pagesAntropologi PesisirDamar Aulia NissaNo ratings yet
- ASMBS Pediatric Metabolic and Bariatric Surgery Guidelines, 2018Document20 pagesASMBS Pediatric Metabolic and Bariatric Surgery Guidelines, 2018Consultorio Pediatria ShaioNo ratings yet
- Ethical Rules For Dentists: (Prescribed by DCI)Document8 pagesEthical Rules For Dentists: (Prescribed by DCI)Khushi DesaiNo ratings yet
- MCL FormatDocument49 pagesMCL Formatasheesh kumarNo ratings yet
- Soapie NjaDocument5 pagesSoapie NjaZhij ConstanteNo ratings yet
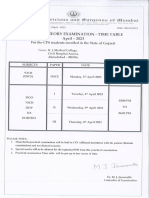
- DCH Time TableDocument1 pageDCH Time TableGane HospitalNo ratings yet
- Cancer Incidence Report 2020Document98 pagesCancer Incidence Report 2020بسام سالمNo ratings yet
- Doh Ao 2008-0008-ADocument2 pagesDoh Ao 2008-0008-AvanceNo ratings yet
- When Doctors Become PatientsDocument2 pagesWhen Doctors Become PatientsJP VdlcNo ratings yet
- CE-marking: Medical and Health Service, ASEAN Tüv Süd PSBDocument8 pagesCE-marking: Medical and Health Service, ASEAN Tüv Süd PSBDuc Nguyen ManhNo ratings yet
- SeptemberDocument36 pagesSeptemberrammvr05No ratings yet
- Letter President Schill 11-7-2022Document10 pagesLetter President Schill 11-7-2022Nalini RajamannanNo ratings yet
- Perception of Covid-19 and Acceptance of Vaccination in Delta State NigeriaDocument27 pagesPerception of Covid-19 and Acceptance of Vaccination in Delta State NigeriaBlessing O. JosiahNo ratings yet
- Dr. Adeeb RizviDocument8 pagesDr. Adeeb RizviSennen DesouzaNo ratings yet
- Overview of Smoking Cessation Management in Adults - UpToDateDocument20 pagesOverview of Smoking Cessation Management in Adults - UpToDateSalo MarianoNo ratings yet
- James Lorenz B. Felizarte: Personal DataDocument8 pagesJames Lorenz B. Felizarte: Personal DataClifford Dwight RicanorNo ratings yet
- I Great Medi Care Pds enDocument6 pagesI Great Medi Care Pds enainafaqeeraNo ratings yet
- Krishna Kishore Hazarika ProjectDocument76 pagesKrishna Kishore Hazarika ProjectNageshwar SinghNo ratings yet
- Ethiopia School Health Program Framework August 2017 - FINALDocument118 pagesEthiopia School Health Program Framework August 2017 - FINALKeneniNo ratings yet
- Albuterol-Budesonide Fixed-Dose Combination Rescue Inhaler For AsthmaDocument13 pagesAlbuterol-Budesonide Fixed-Dose Combination Rescue Inhaler For AsthmaLydia ? Raposo MartinezNo ratings yet
- Innovations PPT SakthiDocument64 pagesInnovations PPT SakthiSakthi DeviNo ratings yet
- ST - Ann'S College of Nursing, Vijayawada Programme Study Centre-33009 (P) Master Rotation Plan - BPCCHNDocument3 pagesST - Ann'S College of Nursing, Vijayawada Programme Study Centre-33009 (P) Master Rotation Plan - BPCCHNRaniNo ratings yet
- AmysaDocument14 pagesAmysaawanisfauzi90No ratings yet
- Family-Centered Health PromotionDocument5 pagesFamily-Centered Health PromotionGulfam NasrinNo ratings yet
- National Strategy For Obstetric Fistula, 2017-2022Document40 pagesNational Strategy For Obstetric Fistula, 2017-2022Faisal Mohammad AhamedNo ratings yet