You might also like
- Wiring Diagram-Split System Air ConditionerDocument1 pageWiring Diagram-Split System Air ConditionerSohail Ejaz Mirza85% (13)
- Electrical Conduits & Fittings: Protect Electrical Cables and WiresDocument18 pagesElectrical Conduits & Fittings: Protect Electrical Cables and WiresA Ma RaahNo ratings yet
- Wildlife Fact File - Mammals - Pgs. 251-260Document20 pagesWildlife Fact File - Mammals - Pgs. 251-260ClearMind84100% (3)
- Ujian Lokal MCQDocument23 pagesUjian Lokal MCQAnnissa Syaira100% (2)
- 2.ITP For Excavation & Laying of 33kV & FO CableDocument2 pages2.ITP For Excavation & Laying of 33kV & FO Cabletahirsaleem100% (1)
- Periapan Ujian MRCOG Fetal MedicineDocument224 pagesPeriapan Ujian MRCOG Fetal MedicineAnnissa Syaira100% (1)
- Bimarker Aswin BoyDocument10 pagesBimarker Aswin BoyAswin BoyNo ratings yet
- P Selectin 2Document7 pagesP Selectin 2DesyHandayaniNo ratings yet
- Placental Growth Factor in Pre-Eclampsia: Friend or Foe?: NephrologydigestDocument3 pagesPlacental Growth Factor in Pre-Eclampsia: Friend or Foe?: NephrologydigestLuciana PietroNo ratings yet
- A Novel Human-Specific Soluble Vascular Endothelial Growth Factor Receptor 1Document21 pagesA Novel Human-Specific Soluble Vascular Endothelial Growth Factor Receptor 1edelinNo ratings yet
- Chronic Kidney Disease May Be Differentially Diagnosed From Preeclampsia by Serum BiomarkersDocument5 pagesChronic Kidney Disease May Be Differentially Diagnosed From Preeclampsia by Serum BiomarkersmeliabudiNo ratings yet
- Ajpheart 00045 2018Document15 pagesAjpheart 00045 2018kamkamNo ratings yet
- 17189.1 20150302091114 CoveredDocument11 pages17189.1 20150302091114 CoveredLintang SuroyaNo ratings yet
- A Cross Sectional Study To Assess The SFLT - 1:PlGF Ratio in Pregnant Women With and Without PreeclampsiaDocument8 pagesA Cross Sectional Study To Assess The SFLT - 1:PlGF Ratio in Pregnant Women With and Without PreeclampsiaEvita LarasNo ratings yet
- PLGF, sFlt-1 and sFlt-1/PlGF Ratio: Promising Markers For Predicting Pre-EclampsiaDocument6 pagesPLGF, sFlt-1 and sFlt-1/PlGF Ratio: Promising Markers For Predicting Pre-EclampsiaPeertechz Publications Inc.No ratings yet
- Pre-Eclampsia Prediction Panel - Anatomy, Etymology and AnalysisDocument1 pagePre-Eclampsia Prediction Panel - Anatomy, Etymology and AnalysisSalome Adame GuisadoNo ratings yet
- Novel Therapies For Preeclampsia: Suzanne D. Burke and S. Ananth KarumanchiDocument11 pagesNovel Therapies For Preeclampsia: Suzanne D. Burke and S. Ananth KarumanchiEgi NabilaNo ratings yet
- Excess Placental Soluble Fms-Like Tyrosine Kinase 1 (Sflt1) May Contribute To Endothelial Dysfunction, Hypertension, and Proteinuria in PreeclampsiaDocument10 pagesExcess Placental Soluble Fms-Like Tyrosine Kinase 1 (Sflt1) May Contribute To Endothelial Dysfunction, Hypertension, and Proteinuria in PreeclampsiaEnrique RosasNo ratings yet
- Mechanisms and Potential Therapies For PreeclampsiaDocument8 pagesMechanisms and Potential Therapies For PreeclampsiaAchmad Deza FaristaNo ratings yet
- A-Acta Paediatr 2010 Apr 99 (4) 494-6Document3 pagesA-Acta Paediatr 2010 Apr 99 (4) 494-6Antonio MartinezNo ratings yet
- Hormonal Causes of RPLDocument9 pagesHormonal Causes of RPLHervi LaksariNo ratings yet
- Prediction Using Serum Glycosylated Fibronectin of Imminent Pre Eclampsia in Women With New Onset HypertensionDocument7 pagesPrediction Using Serum Glycosylated Fibronectin of Imminent Pre Eclampsia in Women With New Onset HypertensionWahyudi WirawanNo ratings yet
- VegfDocument7 pagesVegfBerry BancinNo ratings yet
- AJOG Publication, 2015 On GlyFNDocument9 pagesAJOG Publication, 2015 On GlyFNRaghavanNo ratings yet
- Journal Obsgyn 1Document9 pagesJournal Obsgyn 1Slr RandiNo ratings yet
- Hypertensionaha 113 01787Document7 pagesHypertensionaha 113 01787Ayhan CiftciNo ratings yet
- Corto CTCF VegfDocument6 pagesCorto CTCF Vegfunknowncountdown167No ratings yet
- NIH Public Access: Author ManuscriptDocument10 pagesNIH Public Access: Author ManuscriptedelinNo ratings yet
- Hypertension 2011 Woods 94 102 3Document18 pagesHypertension 2011 Woods 94 102 3Nimas Luthfiana HapsariNo ratings yet
- Filosofia Del Cuerpo HumaniDocument14 pagesFilosofia Del Cuerpo HumaniCristina Galvez PerezNo ratings yet
- No 3Document16 pagesNo 3Bian DaraNo ratings yet
- Placental Lactogen As A Marker of Maternal Obesity, Diabetes, and Fetal Growth Abnormalities: Current Knowledge and Clinical PerspectivesDocument19 pagesPlacental Lactogen As A Marker of Maternal Obesity, Diabetes, and Fetal Growth Abnormalities: Current Knowledge and Clinical PerspectivesLigia AbdalaNo ratings yet
- SFLT 1Document10 pagesSFLT 1William Camilo Camargo MartinezNo ratings yet
- HeheDocument7 pagesHeheAlfian BagusNo ratings yet
- Angiogenic Factors in The Pathogenesis and Pathophysiology of Preeclampsia A Mini ReviewDocument7 pagesAngiogenic Factors in The Pathogenesis and Pathophysiology of Preeclampsia A Mini ReviewedelinNo ratings yet
- Prostasin, Proteases, and Preeclampsia.7Document3 pagesProstasin, Proteases, and Preeclampsia.7rachel0301No ratings yet
- New Developments in The Pathogenesis of Preeclampsia: Mihran V. NaljayanDocument12 pagesNew Developments in The Pathogenesis of Preeclampsia: Mihran V. NaljayanRaymond FrazierNo ratings yet
- Tay 2018Document12 pagesTay 2018Habib Budiman AgungNo ratings yet
- Artigo 1 PDFDocument9 pagesArtigo 1 PDFLarissa F SNo ratings yet
- 2022 Papers Merged 58 70Document13 pages2022 Papers Merged 58 70Yeannie YapNo ratings yet
- Fleming 2010Document4 pagesFleming 2010Ahmed GhanimNo ratings yet
- 14-Uteroplacental Ischemia Results in Proteinuric Hypertension and Elevated SFLT-1Document8 pages14-Uteroplacental Ischemia Results in Proteinuric Hypertension and Elevated SFLT-1ari chandra ervinaNo ratings yet
- Mini-Review: Elizabeth Phipps, Devika Prasanna, Wunnie Brima, and Belinda JimDocument9 pagesMini-Review: Elizabeth Phipps, Devika Prasanna, Wunnie Brima, and Belinda JimemilyNo ratings yet
- Birdir - J Matern Fetal Neonatal Med - 2017Document7 pagesBirdir - J Matern Fetal Neonatal Med - 2017Sayedur RahmanNo ratings yet
- Aspirin in LupusDocument8 pagesAspirin in Lupusyosua simarmataNo ratings yet
- Schramm 2014Document9 pagesSchramm 2014bayuwinotoNo ratings yet
- Chaiworapongsa 2004Document7 pagesChaiworapongsa 2004Lintang SuroyaNo ratings yet
- Angiogenic and Antiangiogenic Factor in AIPDocument50 pagesAngiogenic and Antiangiogenic Factor in AIPberylianamayaNo ratings yet
- 1 s2.0 S0143400421006500 MainDocument8 pages1 s2.0 S0143400421006500 MainEunike KaramoyNo ratings yet
- Jurnal 2Document9 pagesJurnal 2unie cantiqNo ratings yet
- Hypertensionaha 116 08620Document8 pagesHypertensionaha 116 08620Adzkia_ZRNo ratings yet
- BSBT612 19.03.2020 Unit 5Document5 pagesBSBT612 19.03.2020 Unit 5Siddhant SoniNo ratings yet
- Lawrenz 2019Document6 pagesLawrenz 2019angelNo ratings yet
- Maynard ACKD 2019 Pregnancy in Women With Systematic or Nephritis LupusDocument8 pagesMaynard ACKD 2019 Pregnancy in Women With Systematic or Nephritis LupusBCR ABLNo ratings yet
- Ihc 2Document5 pagesIhc 2DesyHandayaniNo ratings yet
- P45NF-E2 Represses Gcm1 in Trophoblast Cells To ReDocument13 pagesP45NF-E2 Represses Gcm1 in Trophoblast Cells To ReM KashifNo ratings yet
- Endocrine Gland-Derived Endothelial Growth Factor (EG-VEGF) Is A Potential Novel Regulator of Human ParturitionDocument10 pagesEndocrine Gland-Derived Endothelial Growth Factor (EG-VEGF) Is A Potential Novel Regulator of Human ParturitionSoad BadawNo ratings yet
- Progesterone in Prevention of PreeclampsiaDocument12 pagesProgesterone in Prevention of PreeclampsiaVishal WahaneNo ratings yet
- Maternal Levels of Growth Differentiation Factor-15 in Patients With PreeclampsiaDocument6 pagesMaternal Levels of Growth Differentiation Factor-15 in Patients With PreeclampsiaqvldNo ratings yet
- NIH Public Access: Author ManuscriptDocument15 pagesNIH Public Access: Author ManuscriptPriyaaNo ratings yet
- 1 s2.0 S2589933323003452 MainDocument10 pages1 s2.0 S2589933323003452 MainimedamNo ratings yet
- Mini-Review: Elizabeth Phipps, Devika Prasanna, Wunnie Brima, and Belinda JimDocument10 pagesMini-Review: Elizabeth Phipps, Devika Prasanna, Wunnie Brima, and Belinda JimemilyNo ratings yet
- Bmri2020 4808072Document10 pagesBmri2020 4808072nelvianti nelsonNo ratings yet
- Diagnostic Accuracy of SFlt1PlGF Ratio As A MarkerDocument7 pagesDiagnostic Accuracy of SFlt1PlGF Ratio As A MarkerWahyudi WirawanNo ratings yet
- Altered Angiogenesis As A Common Mechanism Underlying Preterm Birth, Small For Gestational Age, and Stillbirth in Women Living With HIVDocument17 pagesAltered Angiogenesis As A Common Mechanism Underlying Preterm Birth, Small For Gestational Age, and Stillbirth in Women Living With HIVMuhammad Pebri Nilhakim ZavbmNo ratings yet
- Persiapan Ujian MRCOG Clinical AssessmentDocument280 pagesPersiapan Ujian MRCOG Clinical AssessmentAnnissa SyairaNo ratings yet
- DocumentDocument11 pagesDocumentAnnissa SyairaNo ratings yet
- s12884 014 0425 8Document17 pagess12884 014 0425 8Annissa SyairaNo ratings yet
- Onset and Persistence of Postpartum Depression in An Inner-City Maternal Health Clinic SystemDocument8 pagesOnset and Persistence of Postpartum Depression in An Inner-City Maternal Health Clinic SystemAnnissa SyairaNo ratings yet
- A Descriptive Model of Preventability in Maternal Morbidity and MortalityDocument6 pagesA Descriptive Model of Preventability in Maternal Morbidity and MortalityAnnissa SyairaNo ratings yet
- Iecex Sir 12.0100XDocument17 pagesIecex Sir 12.0100XFrancesco_CNo ratings yet
- Ceb A 72-3247Document4 pagesCeb A 72-3247turboshaftNo ratings yet
- Essays For Ielts & TOEFLDocument254 pagesEssays For Ielts & TOEFLAnthal Nepal100% (5)
- Odb CdiDocument644 pagesOdb CdiPaul JagdharryNo ratings yet
- Navigating Complexity in Policy ImplementationDocument16 pagesNavigating Complexity in Policy Implementationwab91No ratings yet
- 2 A Performance-Based Approach To Security and Blast-Mitigating Building DesignDocument22 pages2 A Performance-Based Approach To Security and Blast-Mitigating Building DesignVulebg VukoicNo ratings yet
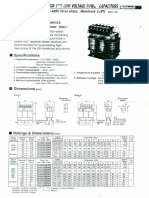
- Series Reactor Lok' V TAG Capacitors: 200 230V / 380-460V Three Phase Eact Nce L 6%Document2 pagesSeries Reactor Lok' V TAG Capacitors: 200 230V / 380-460V Three Phase Eact Nce L 6%bcqbaoNo ratings yet
- Acute Bronchitis: Clinical PearlDocument9 pagesAcute Bronchitis: Clinical PearlLauraNo ratings yet
- 2008 04 Gasoline Pipeline Damaged by Construction Causes FireDocument1 page2008 04 Gasoline Pipeline Damaged by Construction Causes FireHarshad SolankiNo ratings yet
- Complementary Therapies in Medicine: ReviewDocument7 pagesComplementary Therapies in Medicine: ReviewHielmy Auliya HasyimNo ratings yet
- NSTP Action Plan-1Document2 pagesNSTP Action Plan-1Jee En BeeNo ratings yet
- Century Vemap PDFDocument5 pagesCentury Vemap PDFMaster MirrorNo ratings yet
- Wordsworth Graphic Organizer BDocument4 pagesWordsworth Graphic Organizer Bkendall everettNo ratings yet
- Reproductive ImmunologyDocument47 pagesReproductive ImmunologyDavid ChristianNo ratings yet
- VAL 170401 BMAA VAL Activity 2 VMP TemplateDocument17 pagesVAL 170401 BMAA VAL Activity 2 VMP TemplateMohammed S.Gouda100% (1)
- FINAL EXAMINATION in Analytical Chemistry Name: - Yr & Sec: - DateDocument3 pagesFINAL EXAMINATION in Analytical Chemistry Name: - Yr & Sec: - DateDivine Grace ValenzuelaNo ratings yet
- Dokumen - Tips 2 Myanmar Agriculture Sector 3 The Most Important CropsDocument69 pagesDokumen - Tips 2 Myanmar Agriculture Sector 3 The Most Important CropsHan Htun OoNo ratings yet
- Situatie Startup-Uri Start-Up Nation (POCU)Document37 pagesSituatie Startup-Uri Start-Up Nation (POCU)Razvan CosmaNo ratings yet
- Surgical Correction Subglottic Stenosis of The Larynx: AnnoldDocument6 pagesSurgical Correction Subglottic Stenosis of The Larynx: Annoldcanndy202No ratings yet
- Lecture 5Document15 pagesLecture 5Isuru jayaweeraNo ratings yet
- Peterson Content Worth Having: ContentsDocument8 pagesPeterson Content Worth Having: ContentsMuhammet Fatih CantepeNo ratings yet
- Henson, 2001Document24 pagesHenson, 2001maciel27No ratings yet
- Police Injury Pensions - Home Office Guidance To PMABs - Permanent DisablementDocument4 pagesPolice Injury Pensions - Home Office Guidance To PMABs - Permanent DisablementwdtkNo ratings yet
- VaristorsDocument56 pagesVaristorsvalentinlupascu33No ratings yet
- Manual For Quality Seed Production in Wheat.: January 2014Document74 pagesManual For Quality Seed Production in Wheat.: January 2014astuteNo ratings yet
- Syllabus F19Document3 pagesSyllabus F19JRock555No ratings yet