You might also like
- Prediabetes: Why Should We Care?: Ashkan Zand, M.D. Karim Ibrahim, M.D. Bhargavi Patham, M.DDocument9 pagesPrediabetes: Why Should We Care?: Ashkan Zand, M.D. Karim Ibrahim, M.D. Bhargavi Patham, M.DCharlotte KeckhutNo ratings yet
- Relationship Between Malnutrition-Inflammation Complex Syndrome and Fluid Balance in Maintenance Hemodialysis PatientsDocument8 pagesRelationship Between Malnutrition-Inflammation Complex Syndrome and Fluid Balance in Maintenance Hemodialysis PatientsMaricic MilovanNo ratings yet
- Diabetes Mellitus Control Among Elderly Patients at Geriatric Polyclinic of Karangasem District Hospital, Bali, Indonesia: A Preliminary StudyDocument7 pagesDiabetes Mellitus Control Among Elderly Patients at Geriatric Polyclinic of Karangasem District Hospital, Bali, Indonesia: A Preliminary StudyNovita triska dewiNo ratings yet
- Dialysis Induced Hypoglycemia in Non-Diabetic Chronic Kidney Disease PatientsDocument3 pagesDialysis Induced Hypoglycemia in Non-Diabetic Chronic Kidney Disease Patientsscience worldNo ratings yet
- Poster Cardio 1Document2 pagesPoster Cardio 1api-522428594No ratings yet
- Preventing Cardiovascular Disease in Patients With.2 PDFDocument3 pagesPreventing Cardiovascular Disease in Patients With.2 PDFbacharelado2010No ratings yet
- Jurnal DiabetesDocument7 pagesJurnal DiabetesraniedhaNo ratings yet
- Alicia_Paper1Document7 pagesAlicia_Paper1Andrés Thiele HortaNo ratings yet
- Richardson2021 Article L-typeCalciumChannelBlockerUseDocument9 pagesRichardson2021 Article L-typeCalciumChannelBlockerUsetrikusumaNo ratings yet
- Peri Implant Conditions and Levels of Advanced Glycation End Products Among Patients With Different Glycemic ControlDocument7 pagesPeri Implant Conditions and Levels of Advanced Glycation End Products Among Patients With Different Glycemic ControlBagis Emre GulNo ratings yet
- Hispanica L.) Improves Major andDocument7 pagesHispanica L.) Improves Major andapi-42224054No ratings yet
- Sarc X Con 2Document6 pagesSarc X Con 2Samuel SilvaNo ratings yet
- EndocrinoDocument15 pagesEndocrinoMichelle ElizaldeNo ratings yet
- Temple2018 - Mediterranean DietDocument4 pagesTemple2018 - Mediterranean DietAndreea MihalacheNo ratings yet
- Anemia JournalDocument5 pagesAnemia JournalKalyani SanthoshNo ratings yet
- Studi Kasus Asuhan Gizi Pada Pasien Stroke Hemipareses Dekstra Di Rumah Sakit Khusus Daerah Dadi Provinsi Sulawesi SelatanDocument7 pagesStudi Kasus Asuhan Gizi Pada Pasien Stroke Hemipareses Dekstra Di Rumah Sakit Khusus Daerah Dadi Provinsi Sulawesi SelatanGalih MartinNo ratings yet
- 20-4-537Document8 pages20-4-537AzielNo ratings yet
- Glycosylated ProteinsDocument5 pagesGlycosylated ProteinsRonyNo ratings yet
- Factors Predicting Malnutrition in Hemodialysis Patients: A Cross-Sectional StudyDocument10 pagesFactors Predicting Malnutrition in Hemodialysis Patients: A Cross-Sectional StudyMarco TolentinoNo ratings yet
- CKD 6Document8 pagesCKD 6Khusnu Waskithoningtyas NugrohoNo ratings yet
- Prevalence, Risk Factors, Adherence and Non Adherence in Patient With Chronic Kidney Disease: A Prospective StudyDocument7 pagesPrevalence, Risk Factors, Adherence and Non Adherence in Patient With Chronic Kidney Disease: A Prospective StudyRanitaRahmaniarNo ratings yet
- Comparison of Cystic Fibrosis - Related Diabetes With Type 1 Diabetes Based On A German/Austrian Pediatric Diabetes RegistryDocument8 pagesComparison of Cystic Fibrosis - Related Diabetes With Type 1 Diabetes Based On A German/Austrian Pediatric Diabetes RegistryAgus SetiawanNo ratings yet
- Chapter 11: Hypertension, Chronic Kidney Disease, and The ElderlyDocument5 pagesChapter 11: Hypertension, Chronic Kidney Disease, and The ElderlyBudi KhangNo ratings yet
- Efectos de La Suplementación Oral en Pacientes en HD Con MalnutriciónDocument7 pagesEfectos de La Suplementación Oral en Pacientes en HD Con MalnutriciónCarlos Miguel Mendoza LlamocaNo ratings yet
- Fendo 13 885516Document7 pagesFendo 13 885516adri20121989No ratings yet
- Effects of Diet and Exercise in Preventing NIDDM in People With Impaired Glucose ToleranceDocument8 pagesEffects of Diet and Exercise in Preventing NIDDM in People With Impaired Glucose ToleranceOzan OcakNo ratings yet
- Blood Pressure Management in Patients With DiabetesDocument8 pagesBlood Pressure Management in Patients With DiabetesHoài ThươngNo ratings yet
- Article Sciemce90.fullDocument2 pagesArticle Sciemce90.fullHshdhdNo ratings yet
- Association Between The Level of Quality of Life and Nutritional Status in Patients Undergoing Chronic Renal HemodialysisDocument10 pagesAssociation Between The Level of Quality of Life and Nutritional Status in Patients Undergoing Chronic Renal HemodialysisVione rizkiNo ratings yet
- Risk Factors Associated With Type 2 Diabetes Mellitus and The Frequency of Nafld Affected PatientsDocument5 pagesRisk Factors Associated With Type 2 Diabetes Mellitus and The Frequency of Nafld Affected PatientsIJAR JOURNALNo ratings yet
- Additive Effect of Sarcopenia and Anemia On The 10-Year Risk of Diab PDFDocument9 pagesAdditive Effect of Sarcopenia and Anemia On The 10-Year Risk of Diab PDFAfonsoNo ratings yet
- Intradialytic Hypertension in End Stage Renal Disease Patient: Prevalence and Clinical CharacteristicDocument6 pagesIntradialytic Hypertension in End Stage Renal Disease Patient: Prevalence and Clinical CharacteristicAmalNo ratings yet
- Case Report: 17-Year-Old Boy With Renal Failure and The Highest Reported Creatinine in Pediatric LiteratureDocument5 pagesCase Report: 17-Year-Old Boy With Renal Failure and The Highest Reported Creatinine in Pediatric LiteratureYunika ArumNo ratings yet
- Tayem PDFDocument8 pagesTayem PDFCynthia MelindaNo ratings yet
- Frequency and Predictors of Hypoglycemia in Type 2.9Document7 pagesFrequency and Predictors of Hypoglycemia in Type 2.9Doménica JayaNo ratings yet
- Obesidad y CirrosisDocument14 pagesObesidad y CirrosisMarly Tatiana Oviedo CaliNo ratings yet
- Clinical Epidemiology and Global Health: Original ArticleDocument4 pagesClinical Epidemiology and Global Health: Original Articleinnani wildaniaNo ratings yet
- T1DM Commentary Pediatrics 2018Document4 pagesT1DM Commentary Pediatrics 2018GlowstarNo ratings yet
- Nutritional Status in Patients With Diabetes and Chronic Kidney Disease: A Prospective StudyDocument6 pagesNutritional Status in Patients With Diabetes and Chronic Kidney Disease: A Prospective StudyHenry HadiantoNo ratings yet
- 2019 JCEM Primary Prevention of ASCVD and T2DM in Patients at Metabolic RiskDocument47 pages2019 JCEM Primary Prevention of ASCVD and T2DM in Patients at Metabolic Riskguanyulin01No ratings yet
- S0022347621003152Document8 pagesS0022347621003152Vedith KumarNo ratings yet
- InsulinaDocument8 pagesInsulinaClaudiu SufleaNo ratings yet
- Effect of Variability of Hemoglobin Value On Type and Severity of Diabetic Retinopathy in Adult Type II Diabetes Mellitus PatientsDocument11 pagesEffect of Variability of Hemoglobin Value On Type and Severity of Diabetic Retinopathy in Adult Type II Diabetes Mellitus PatientsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Comorbidities in Patients With Gout in R f99b8513Document3 pagesComorbidities in Patients With Gout in R f99b8513Natasya SaraswatiNo ratings yet
- JDR2019 7825804Document9 pagesJDR2019 7825804Anonymous Xc7NwZzoNo ratings yet
- Adiponectin Levels in Non-Obese First-Degree Relatives of Type 2 Diabetes Patients and Non-Diabetic Subjects: A 5-Year Follow-Up StudyDocument11 pagesAdiponectin Levels in Non-Obese First-Degree Relatives of Type 2 Diabetes Patients and Non-Diabetic Subjects: A 5-Year Follow-Up StudyMuhammad Yusuf HanifNo ratings yet
- ADO in BRCDocument10 pagesADO in BRCVlahtNo ratings yet
- Rado SD-2019-MRI-based Assessment and Characterization of Epicardial andDocument10 pagesRado SD-2019-MRI-based Assessment and Characterization of Epicardial andASIK1144No ratings yet
- Clinical Course of Diabetic Ketoacidosis in Hypertriglyceridemic Pancreatitis Pancreas 2015Document4 pagesClinical Course of Diabetic Ketoacidosis in Hypertriglyceridemic Pancreatitis Pancreas 2015América FloresNo ratings yet
- Estimation of Lipid Profile and Glycemic Status and Liver Enzymes, Among Patients With Non-Alcoholic Fatty Liver DiseaseDocument13 pagesEstimation of Lipid Profile and Glycemic Status and Liver Enzymes, Among Patients With Non-Alcoholic Fatty Liver DiseaseIJAR JOURNALNo ratings yet
- 1 s2.0 S0002870320302143 MainDocument9 pages1 s2.0 S0002870320302143 MaindeepNo ratings yet
- Glycemic index, glycemic load, and blood pressure meta-analysisDocument15 pagesGlycemic index, glycemic load, and blood pressure meta-analysisLisiane PerinNo ratings yet
- A Study of Steroid-Induced Diabetes Mellitus in Leprosy: Original ArticleDocument5 pagesA Study of Steroid-Induced Diabetes Mellitus in Leprosy: Original Articlecitra deriyaNo ratings yet
- 0104 1169 Rlae 28 E3369Document10 pages0104 1169 Rlae 28 E3369surya rakhmat hidayatNo ratings yet
- fsn3 1642Document11 pagesfsn3 1642Umi RianaNo ratings yet
- 17 Malenica 920 ADocument7 pages17 Malenica 920 AqiraniNo ratings yet
- Prevalence of Chronic Kidney Disease in Patients With or at A High Risk of Cardiovascular DiseaseDocument4 pagesPrevalence of Chronic Kidney Disease in Patients With or at A High Risk of Cardiovascular DiseasenuvitaNo ratings yet
- Protein Energy Malnutrition in CKD PatientsDocument4 pagesProtein Energy Malnutrition in CKD PatientsEditor IJTSRDNo ratings yet
- Acute Kidney Injury and Diabetic Ketoacidosis in Pediatric Patients: Risk FactorsDocument4 pagesAcute Kidney Injury and Diabetic Ketoacidosis in Pediatric Patients: Risk FactorsMarcelliaNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 8: UrologyFrom EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyRating: 3 out of 5 stars3/5 (1)
- Noncompartment Model - Pharmacokinetics: DR C. V. S. SubrahmanyamDocument44 pagesNoncompartment Model - Pharmacokinetics: DR C. V. S. SubrahmanyamBandameedi RamuNo ratings yet
- Hyperthyroidism, Thyroid Storm, and Graves Disease: BackgroundDocument22 pagesHyperthyroidism, Thyroid Storm, and Graves Disease: BackgroundAnonymous 3OoumAUytNo ratings yet
- 40 Normal Labor and DystociaDocument47 pages40 Normal Labor and DystociaCitra Wulandari SofyanNo ratings yet
- Hotel Spa and Wellness Services in Crete: A Marketing AnalysisDocument6 pagesHotel Spa and Wellness Services in Crete: A Marketing AnalysisestherNo ratings yet
- Urinary Bladder MassDocument2 pagesUrinary Bladder Masskarl de guzmanNo ratings yet
- Asthma Lesson PlanDocument26 pagesAsthma Lesson PlanBharat Singh BanshiwalNo ratings yet
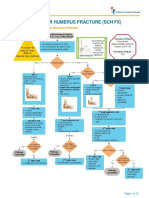
- Fracture Supracondylar HumerusDocument12 pagesFracture Supracondylar HumeruskemsNo ratings yet
- ASSESSMENT DIAGNOSIS PLANNING EVALUATIONDocument2 pagesASSESSMENT DIAGNOSIS PLANNING EVALUATIONJiraGonzalesNo ratings yet
- Velashape2 BrochureDocument8 pagesVelashape2 BrochureddNo ratings yet
- Dietetics - Unit 1Document4 pagesDietetics - Unit 1maglit777No ratings yet
- Firstaid Test 2001Document10 pagesFirstaid Test 2001Rinor MujajNo ratings yet
- Dr. Craig Childress: DSM-5 Diagnosis of "Parental Alienation" ProcessesDocument10 pagesDr. Craig Childress: DSM-5 Diagnosis of "Parental Alienation" ProcessesParentalAlienationDynamics75% (4)
- Diabetes MellitusDocument75 pagesDiabetes MellitusIndika KarunamuniNo ratings yet
- Fistula in AnoDocument21 pagesFistula in AnoHannah LeiNo ratings yet
- Tai Chi Companion Part 1 - Getting StartedDocument18 pagesTai Chi Companion Part 1 - Getting Startedradical5770100% (1)
- NMAT REVIEWER: DEFENSE MECHANISMSDocument2 pagesNMAT REVIEWER: DEFENSE MECHANISMSEllah Gutierrez100% (1)
- Practice: Orthodontics. Part 1: Who Needs Orthodontics?Document5 pagesPractice: Orthodontics. Part 1: Who Needs Orthodontics?Alejandra MoralesNo ratings yet
- Medical Records Audit ChecklistDocument2 pagesMedical Records Audit ChecklistSrinivas Polikepati93% (42)
- Adolesent Drugs PDFDocument767 pagesAdolesent Drugs PDFAlbghdadi CristianNo ratings yet
- Levofloxacin in Typhoid FeverDocument4 pagesLevofloxacin in Typhoid FeverUsman HanifNo ratings yet
- Template - Case Report ArticleDocument4 pagesTemplate - Case Report Articlegerald randyNo ratings yet
- Personal Notes While at McLeanDocument12 pagesPersonal Notes While at McLeanmcleanhospitalNo ratings yet
- Case Study and Research On EMDR For Combat PTSDDocument21 pagesCase Study and Research On EMDR For Combat PTSDDaniel R. Gaita, MA, LMSWNo ratings yet
- Caregiving 8 Periodical ExamDocument3 pagesCaregiving 8 Periodical ExamLeizette Zuniga Tacang95% (22)
- NCP Pain (H Mole)Document3 pagesNCP Pain (H Mole)Khat Quimen Mayo86% (7)
- Attending Physicians Statement Crisis Cover Renal Failure - 041222Document2 pagesAttending Physicians Statement Crisis Cover Renal Failure - 041222max leeNo ratings yet
- Accepted Manuscript: Complementary Therapies in MedicineDocument24 pagesAccepted Manuscript: Complementary Therapies in MedicineAndrea BarresiNo ratings yet
- Synergistic Activation of Doxorubicin Against Cancer: A ReviewDocument6 pagesSynergistic Activation of Doxorubicin Against Cancer: A ReviewArya GuganNo ratings yet
- Lotus Theory: Author: Published OnDocument7 pagesLotus Theory: Author: Published OnDilip Kininge100% (1)
- The Management of Pressure Ulcers in Primary and Secondary Care PDFDocument464 pagesThe Management of Pressure Ulcers in Primary and Secondary Care PDFDragos-Ronald RugescuNo ratings yet